Concurrent Invasive Ductal Carcinoma of the Breast and Malignant Follicular Lymphoma, Initially Suspected to Be Metastatic Breast Cancer: A Case Report
- Affiliations
-
- 1Department of Radiology, Kyungpook National University Hospital, Daegu, Korea.
- 2Department of Radiology, Kyungpook National University Medical Center, Daegu, Korea. mamrad@knu.ac.kr
- 3Department of Pathology, Kyungpook National University Medical Center, Daegu, Korea.
- 4Department of Surgery, Kyungpook National University Medical Center, Daegu, Korea.
Abstract
- This report describes a case of a 40-year-old female patient with concurrent invasive ductal carcinoma of the breast and malignant follicular lymphoma, initially suspected to be metastatic breast cancer. During the initial evaluation of invasive ductal carcinoma of right breast, multiple lymphadenopathies were noted throughout the body on ultrasonography and positron emission tomography/computed tomography images. Clinically, metastatic breast cancer was suggested, and the patient was administered chemotherapy, including hormonal therapy. The breast cancer improved slightly, but the lymphadenopathies progressed and excisional biopsy of a cervical lymph node revealed malignant follicular lymphoma.
MeSH Terms
Figure
-
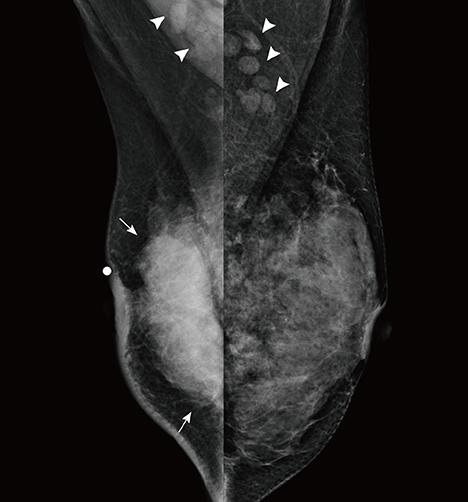
Figure 1 Mammograms of both breasts. Bilateral mediolateral oblique view of mammograms show a large high density mass (arrows) and skin thickening on the right breast and bilateral lymphadenopathies (arrowheads).
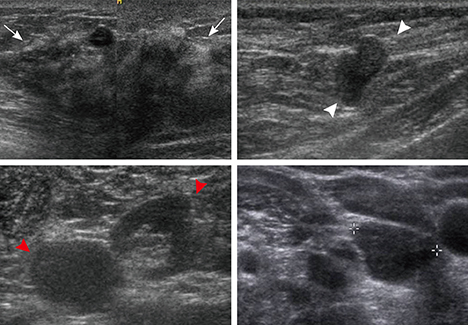
Figure 2 Ultrasonographic (US) images of the right breast cancer and regional lymph nodes. US images reveal an 8 cm irregular hypoechoic mass in the right breast (arrows) and abnormal lymph nodes in the right (white arrowheads) and left axilla (red arrowheads) and the left supraclavicular area (crosses).
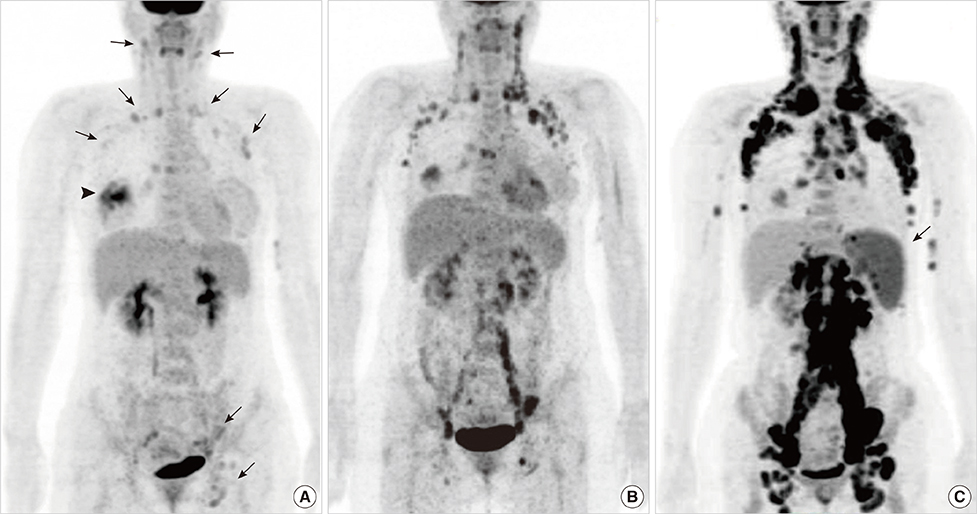
Figure 3 Maximal intensity projection images of positron emission tomography/computed tomography (PET/CT) scans. (A) Maximal intensity projection image of the initial PET/CT scan shows multiple lymphadenopathies with mildly increased 2-[18F]-fluoro-2-deoxy-d-glucose (FDG) uptake in the axillae on both sides, in the neck, and in the left external iliac and inguinal areas (arrows). The arrowhead indicates high FDG uptake in the right breast mass. (B) PET/CT scan after the discontinuation of chemotherapy shows that the systemic lymphadenopathies are aggravated. (C) Follow-up PET/CT scan demonstrates aggravated lymphadenopathies throughout the torso. Note the newly appeared splenomegaly (arrow). Excisional biopsy of a neck lymph node reveals malignant follicular lymphoma.

Figure 4 Histologic images of follicular lymphoma. (A) Hematoxyline and eosin staining photomicrograph of a lymph node shows effaced nodal architecture due to closely packed neoplastic follicles (H&E stain, × 40). Inset: The neoplastic follicles show a monotonous population of cells without germinal center and lack any significant mantle zones (H&E stain, × 400). (B) Bcl-2 immunostaining photomicrograph of a lymph node demonstrates positive in follicular cells. Expression of Bcl-2 oncoprotein by follicular cells is a feature of lymphoma and not reactive follicular center cells (Bcl-2 immunostain, × 100).
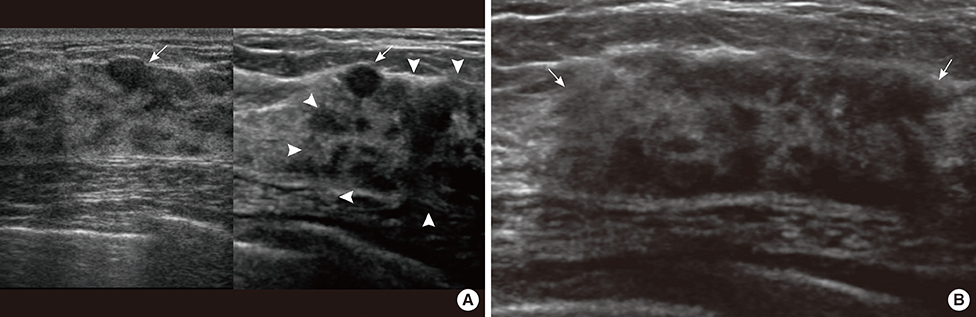
Figure 5 Ultrasonographic (US) images of left breast cancer. (A) On comparison of transverse images of the left breast (left: initial; right: follow-up), US images reveal a benign looking ovoid nodule in the initial and follow-up images (arrows) and a new heterogenous hypoechoic area in the follow-up image (arrowheads). (B) Transverse US image shows a heterogenous hypoechoic area in the left upper outer breast (arrows).

Figure 6 Histologic images of right breast cancer. (A) Hematoxyline and eosin (H&E) staining photomicrograph of right breast cancer shows proliferation of high nuclear grade malignant ductal epithelial cells which represent ductal carcinoma in situ (white arrows) and portions of invasion under basement membrane mean invasive ductal carcinoma (black arrow) (H&E stain, × 40), Inset: Note tumor emboli in lymphatic channels that provide more chance of lymphangitic or hematogenous metastasis (H&E stain, × 40). (B-D) Immunohistochemical staining of surgical specimen is positive for estrogen receptor (×100) (B) and progesterone receptor (×100) (C), equivocal (2+) for human epidermal growth factor receptor 2 (×100) (D). Fluorescence in situ hybridization reveals negativity for HER2 (not shown).
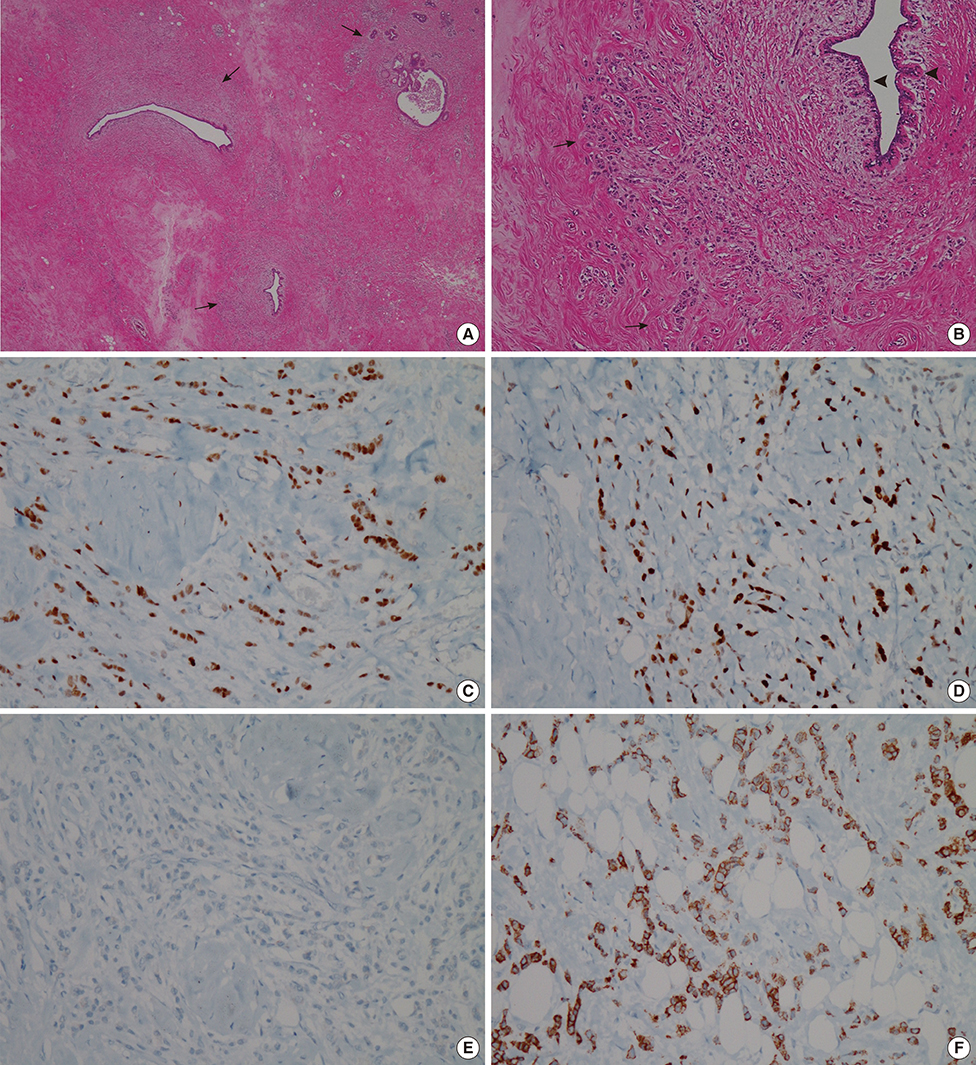
Figure 7 Histologic images of left breast cancer. (A, B) Hematoxyline and eosin (H&E) staining photomicrographs of left breast cancer demonstrate multifocal infiltrative distribution of tumor cells in periductal area under the basement membrane (arrows). Note that normal ductal epithelium without ductal carcinoma in situ component that often accompanies primary cancer (arrowheads) (H&E stain, A: ×20, B: ×100). (C-E) Immunohistochemistry results are positive for estrogen receptor (×100) (C) and progesterone receptor (×100) (D), and negative for human epidermal growth factor receptor 2 (× 100) (E). (F) Immunoperoxidase staining photomicrograph of left breast cancer shows E-cadherin expression that is lost in lobular carcinoma (Immunohistochemical stain for E-cadherin, × 100).
Reference
-
1. Wiernik PH, Hu X, Ratech H, Fineberg S, Marino P, Schleider MA, et al. Non-Hodgkin's lymphoma in women with breast cancer. Cancer J. 2000; 6:336–342.2. Dutta Roy S, Stafford JA, Scally J, Selvachandran SN. A rare case of breast carcinoma co-existing with axillary mantle cell lymphoma. World J Surg Oncol. 2003; 1:27.3. Suresh Attili VS, Dadhich HK, Rao CR, Bapsy PP, Batra U, Anupama G, et al. A case of breast cancer coexisting with B-cell follicular lymphoma. Austral-Asian J Cancer. 2007; 6:155–156.4. Benoit L, Arnould L, Collin F, Fraisse J, Cuisenier J, Chauffert B. Concurrent lymphoma and metastatic breast carcinoma in the axillary, confounding sentinel lymph-node biopsy. Eur J Surg Oncol. 2004; 30:462–463.
Article5. Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998; 11:155–168.6. Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007; 25:118–145.
Article7. Barranger E, Marpeau O, Uzan S, Antoine M. Axillary sentinel node involvement by breast cancer coexisting with B-cell follicular lymphoma in nonsentinel nodes. Breast J. 2005; 11:227–228.
Article8. Pandey U, Naraynan M, Karnik U, Sinha B. Carcinoma metastasis to unexpected synchronous lymphoproliferative disorder: report of three cases and review of literature. J Clin Pathol. 2003; 56:970–971.
Article9. Todd MT, Douglas Y. Bilateral breast cancer. In : Singletary SE, Robb GL, Hortobagyi GN, editors. Advanced Therapy of Breast Disease. 2nd ed. Hamilton: B.C. Decker;2004. p. 629–630.10. Lee SH, Park JM, Kook SH, Han BK, Moon WK. Metastatic tumors to the breast: mammographic and ultrasonographic findings. J Ultrasound Med. 2000; 19:257–262.
Article11. Gupta D, Merino MI, Farhood A, Middleton LP. Metastases to breast simulating ductal carcinoma in situ: report of two cases and review of the literature. Ann Diagn Pathol. 2001; 5:15–20.
Article12. MacNeill M, Arnott I, Thomas J. Fine needle aspiration cytology is a valuable adjunct to axillary ultrasound in the preoperative staging of breast cancer. J Clin Pathol. 2011; 64:42–46.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multifocal Bilateral Breast Cancer and Breast Follicular Lymphoma: A Simple Coincidence?
- Synchronous Presentation of Ductal Carcinoma In Situ of the Breast with Follicular Lymphoma
- Invasive Ductal Carcinoma of the Male Breast: A Case Report and Review of the Literature
- Nodular Metastatic Carcinoma from Invasive Lobular Breast Cancer
- Multiple Primary Malignant Neoplasms: A Case Report of Breast Mucinous Carcinoma and Extramammary Diffuse Large B-Cell Lymphoma in a Male Patient
