Changes in Melanin and Melanocytes in Mottled Hypopigmentation after Low-Fluence 1,064-nm Q-Switched Nd:YAG Laser Treatment for Melasma
- Affiliations
-
- 1Department of Dermatology, Kyungpook National University School of Medicine, Daegu, Korea. hykang@ajou.ac.kr
- 2Department of Dermatology, Ajou University School of Medicine, Suwon, Korea.
- KMID: 2352514
- DOI: http://doi.org/10.5021/ad.2015.27.3.340
Abstract
- No abstract available.
Figure
-
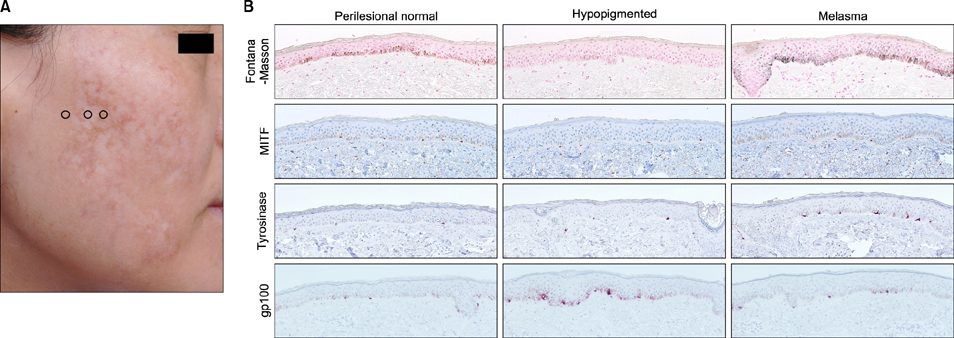
Fig. 1 (A) Mottled hypopigmentation developing after laser toning for melasma treatment in a 41-year-old woman with Fitzpatrick skin type IV. Hypopigmented, hyperpigmented (i.e., melasma), and adjacent perilesional normal skin were evaluated. Circles indicate biopsy sites of perilesional normal (left), hypopigmented (middle), and melasma (right) skin. (B) Histopathologic examination showed melanin pigmentation was markedly reduced in the basal layer of lesional skin (Fontana-Masson staining). The number of melanocytes, determined according to microphthalmia-associated transcription factor (MITF) expression, did not differ much between lesional skin and perilesional normal skin or melasma skin. The expression of gp100 was higher in hypopigmented lesional skin than perilesional normal skin or even melasma skin (×200).

Fig. 2 (A) A 49-year-old woman with Fitzpatrick skin type III presented with typical mottled hypopigmentation after laser toning for 1 year. Circle indicates biopsy sites of the hypopigmented lesion. (B) Lesional skin biopsy showed the complete absence of melanin pigment in hypopigmented skin. However, there was no reduction in the number of melanocytes and rather increased gp100 expression (×200). MITF: microphthalmia-associated transcription factor.
Reference
-
1. Jeong SY, Chang SE, Bak H, Choi JH, Kim IH. New melasma treatment by collimated low fluence Q-switched Nd : YAG laser. Korean J Dermatol. 2008; 46:1163–1170.2. Polnikorn N. Treatment of refractory dermal melasma with the MedLite C6 Q-switched Nd:YAG laser: two case reports. J Cosmet Laser Ther. 2008; 10:167–173.
Article3. Cho SB, Kim JS, Kim MJ. Melasma treatment in Korean women using a 1064-nm Q-switched Nd:YAG laser with low pulse energy. Clin Exp Dermatol. 2009; 34:e847–e850.
Article4. Kim MJ, Kim JS, Cho SB. Punctate leucoderma after melasma treatment using 1064-nm Q-switched Nd:YAG laser with low pulse energy. J Eur Acad Dermatol Venereol. 2009; 23:960–962.
Article5. Kim T, Cho SB, Oh SH. Punctate leucoderma after 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low-fluence therapy: is it melanocytopenic or melanopenic. Dermatol Surg. 2010; 36:1790–1791.
Article6. Ryu HJ, Kim J. A case of mottled hypopigmentation after low-fluence 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser therapy. J Cosmet Laser Ther. 2013; 15:290–292.
Article7. Chan NP, Ho SG, Shek SY, Yeung CK, Chan HH. A case series of facial depigmentation associated with low fluence Q-switched 1,064 nm Nd:YAG laser for skin rejuvenation and melasma. Lasers Surg Med. 2010; 42:712–719.
Article8. Kim HS, Jung HD, Kim HO, Lee JY, Park YM. Punctate leucoderma after low-fluence 1,064-nm quality-switched neodymium-doped yttrium aluminum garnet laser therapy successfully managed using a 308-nm excimer laser. Dermatol Surg. 2012; 38:821–823.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypopigmentation Induced by Frequent Low-Fluence, Large-Spot-Size QS Nd:YAG Laser Treatments
- Treatment of Melasma with the Photoacoustic Twin Pulse Mode of Low-Fluence 1,064 nm Q-Switched Nd:YAG Laser
- A Case of Punctate Leukoderma after 1,064 nm Q-Switched Nd:YAG Laser
- Partial Unilateral Lentiginosis Successfully Treated with a High-fluence 1,064-nm Q-switched Neodymium:Yttriumaluminum-garnet Laser
- Beneficial Effect of Low Fluence 1,064 nm Q-Switched Neodymium:Yttrium-Aluminum-Garnet Laser in the Treatment of Senile Lentigo
