J Korean Acad Prosthodont.
2016 Jul;54(3):286-290. 10.4047/jkap.2016.54.3.286.
Fabrication of palatal lift prosthesis using thermoplastic resin for a patient with velopharyngeal insufficiency
- Affiliations
-
- 1Department of Prosthodontics, School of Dentistry, Yonsei University, Seoul, Republic of Korea. DRYBPARK@yuhs.ac
- KMID: 2344869
- DOI: http://doi.org/10.4047/jkap.2016.54.3.286
Abstract
- Recently, flexible removable prosthesis with thermoplastic resin clasp has increasingly become popular. In comparison with conventionally used acrylic resin, thermoplastic resin has lower flexural strength and elastic modulus. Thus, flexible removable prosthesis has low risk of fracture, so denture base can be made thin and light, increasing patient comfort. Also, it can passively sit at tooth undercut during rest, so abutment teeth need minimum or no preparation. In this case report, a 44 year old female patient with mild velopharyngeal insufficiency was treated with a palatal lift prosthesis made of polyester thermoplastic resin. Since the patient had no missing tooth and desired conservative treatment, the flexible removable prosthesis provided relatively satisfactory results.
MeSH Terms
Figure
-

Fig. 1. Intraoral photos. (A) Maxillary dentition, (B) Mandibular dentition.
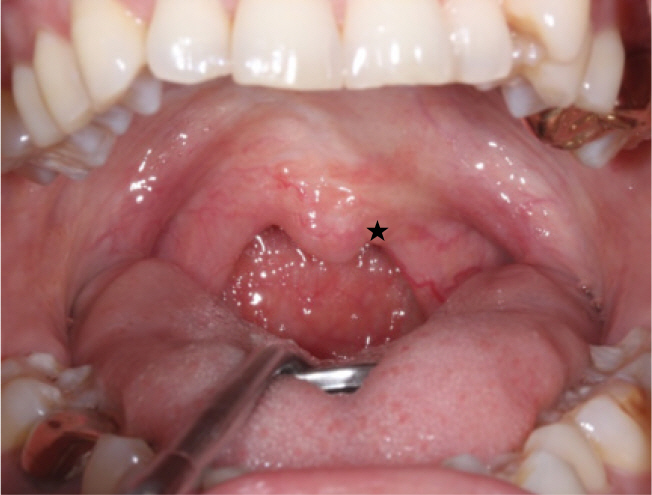
Fig. 2. Intraoral photo during "A" phonation. Star sign shows lower elevation of left soft palate.
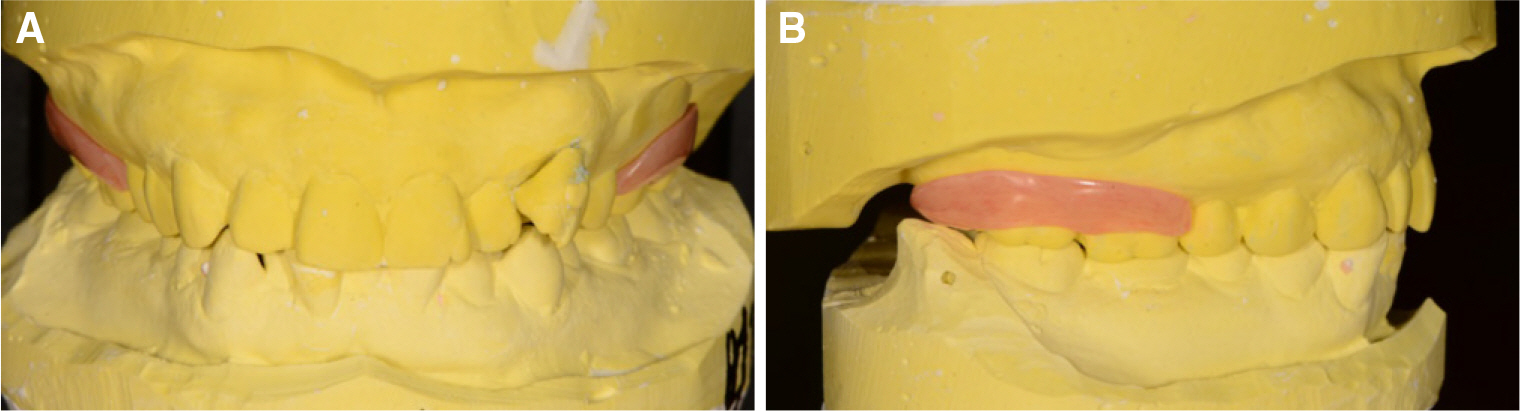
Fig. 3. Mounted casts at CO with a final prosthesis. (A) Front view, (B) Lateral view.
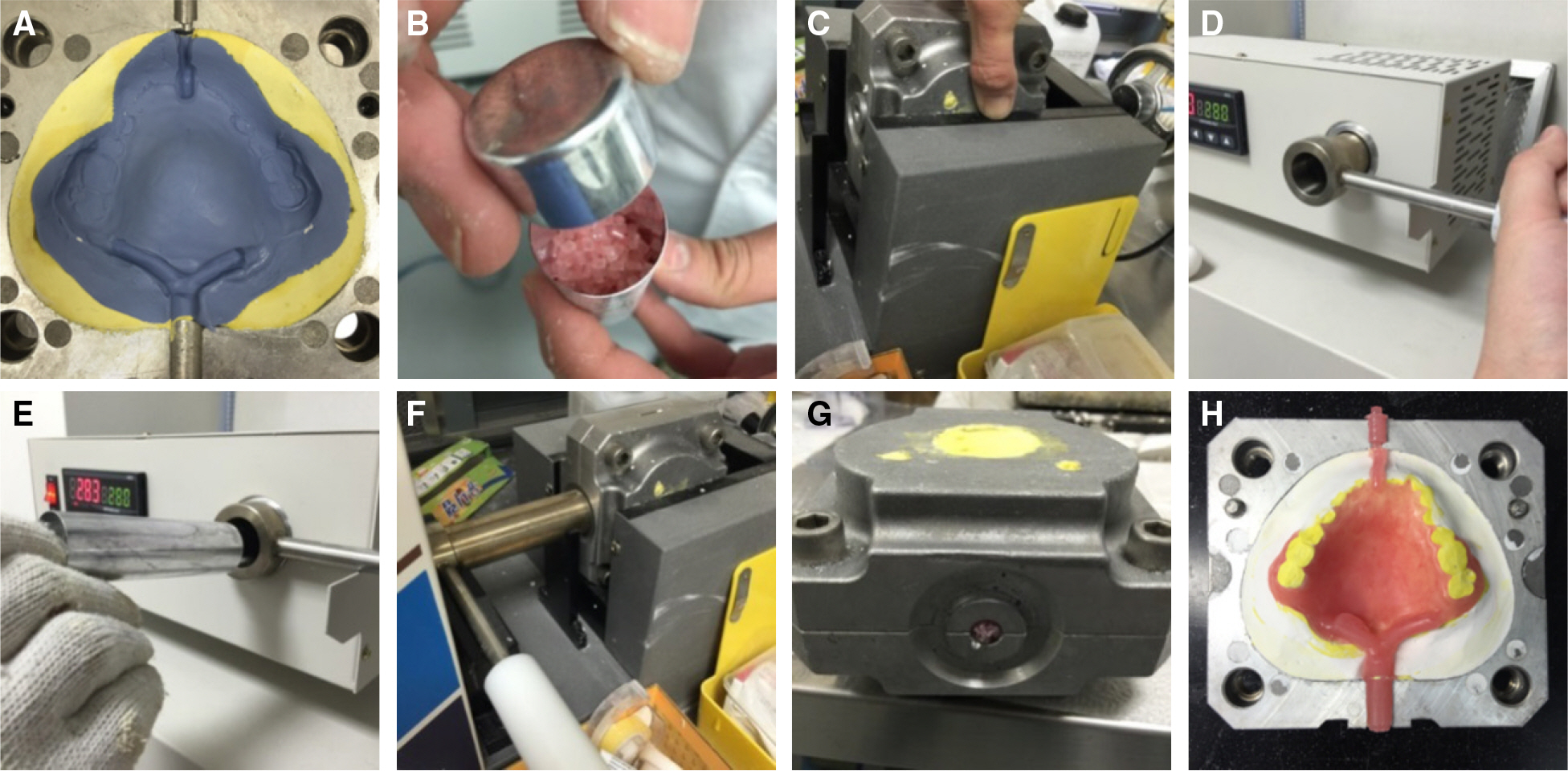
Fig. 4. Flasking & packing process. (A) Putty investment, (B) Thermoplastic pellets, (C) Special flask for injection molding technique, (D, E) Pellets in a cartridge plasticized in an electric furnace, (F) Cartridge placed on the inlet of the flask and compressed, (G) Cooling, (H) Deflasking.

Fig. 5. Palatal lift prosthesis after polishing.

Fig. 6. Delivery.
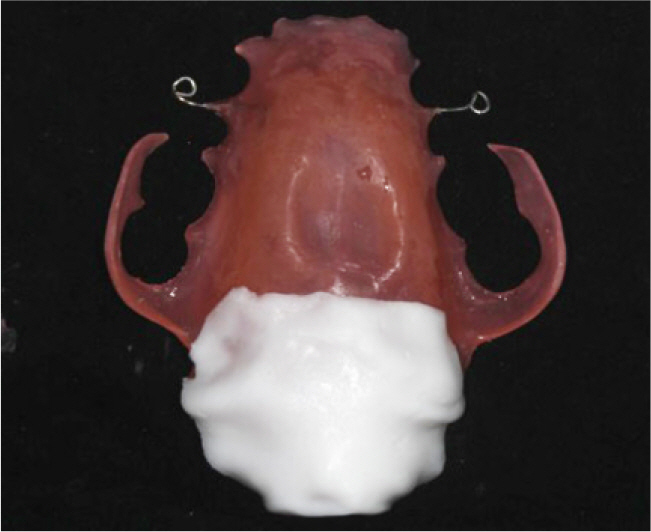
Fig. 7. Prosthesis after relining with Coe-comfort.
Reference
-
1.Johns DF., Rohrich RJ., Awada M. Velopharyngeal incompetence: a guide for clinical evaluation. Plast Reconstr Surg. 2003. 112:1890–7.2.Goudy S., Ingraham C., Canady J. Noncleft velopharyngeal insufficiency: Etiology and need for surgical treatment. Int J Otolaryngol. 2012. 1–3.
Article3.Schneider E., Shprintzen RJ. A survey of speech pathologists: current trends in the diagnosis and management of velopharyngeal insufficiency. Cleft Palate J. 1980. 17:249–53.4.Mazaheri M., Mazaheri EH. Prosthodontic aspects of palatal elevation and palatopharyngeal stimulation. J Prosthet Dent. 1976. 35:319–26.
Article5.La Velle WE., Hardy JC. Palatal lift prostheses for treatment of palatopharyngeal incompetence. J Prosthet Dent. 1979. 42:308–15.6.Kipfmueller LJ., Lang BB. Treating velopharyngeal inadequacies with a palatal lift prosthesis. J Prosthet Dent. 1972. 27:63–72.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interim palatal lift prosthesis as a constituent of multidisciplinary approach in the treatment of velopharyngeal incompetence
- Fabrication of palatal lift prosthesis for a patient with palatal defect
- A Clinical Study of Palatal lift for treatment of velopharyngeal incompetency
- Palatal obturator restoration of a cleft palate patient with velopharyngeal insufficiency: a clinical report
- Velopharyngeal Insufficiency Induced by a Postoperative Palatal Fistula during Articulation Development Period: A Case Report
