Comparative Study between Digital Tomosynthesis and Endoscopic Retrograde Cholangiopancreatography for the Evaluation of Common Bile Duct Stones: Focus on Detection and Stone Conspicuity
- Affiliations
-
- 1Department of Radiology and Medical Research Institute, School of Medicine, Ewha Womans University, Seoul, Korea. bbaek@ewha.ac.kr
- 2Department of Internal Medicine and Medical Research Institute, School of Medicine, Ewha Womans University, Seoul, Korea.
Abstract
- PURPOSE
To compare digital tomosynthesis with endoscopic retrograde cholangiopancreatography (ERCP) for the evaluation of common bile duct (CBD) stones as a complementary diagnostic tool.
MATERIALS AND METHODS
Ninety six consecutive patients clinically suspected of having CBD stones underwent ERCP and digital tomosynthesis over 22 months, from December, 2008 to May, 2010. Fourteen patients were excluded. Therefore 82 patients were included in this study. The images were retrospectively reviewed to compare the results with the final analysis based on the consensus of two abdominal radiologists. An evaluation of the presence of CBD stones was followed by a determination of the margins for the stones, scored with a five-point conspicuity scale.
RESULTS
Among the 82 patients, 54 collectively had 89 CBD stones and 28 had no stones. The sensitivity and specificity for the detection of CBD stones were 91.0% and 80.6% for ERCP, 92.1% and 93.5% for digital tomosynthesis, respectively. The average score was 3.29 for ERCP and 3.89 for digital tomosynthesis in 77 similar detected stones. Digital tomosynthesis demonstrated significantly better conspicuity than ERCP (p = 0.001).
CONCLUSION
Digital tomosynthesis is an effective and complementary diagnostic method for the evaluation of CBD stones.
MeSH Terms
Figure
-
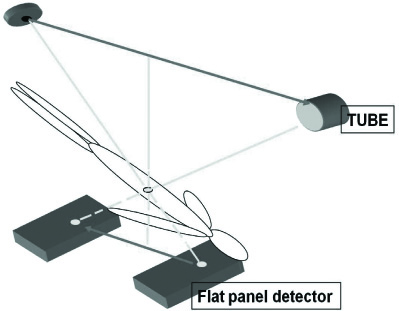
Fig. 1 Mimetic diagram of digital tomosynthesis. Digital tomosynthesis image acquired by continuous fluoroscopic exposure from top to bottom at a range of 40°, and with the target part as the center of the CBD. To focus the CBD, the target point is set at a depth of 120 mm from the skin with 70 mm buffer in all directions and continuous X-ray exposure for 2.5 seconds. Note.-CBD = common bile duct
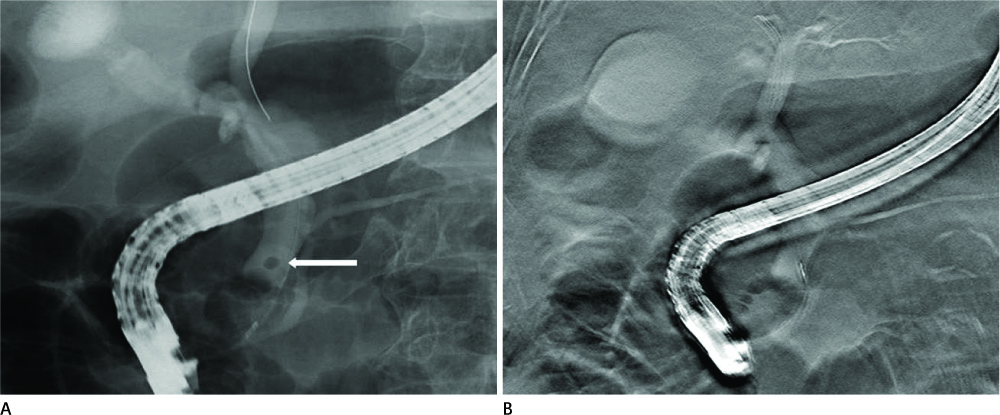
Fig. 2 A 79-year-old man without a CBD stone. A. ERCP image obtained after injection of contrast material showing a CBD stone (arrow), which is considered to be a score of 5. B. Although the digital tomosynthesis image is slightly blurred, no definite stones are seen in the CBD. Note.-CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography
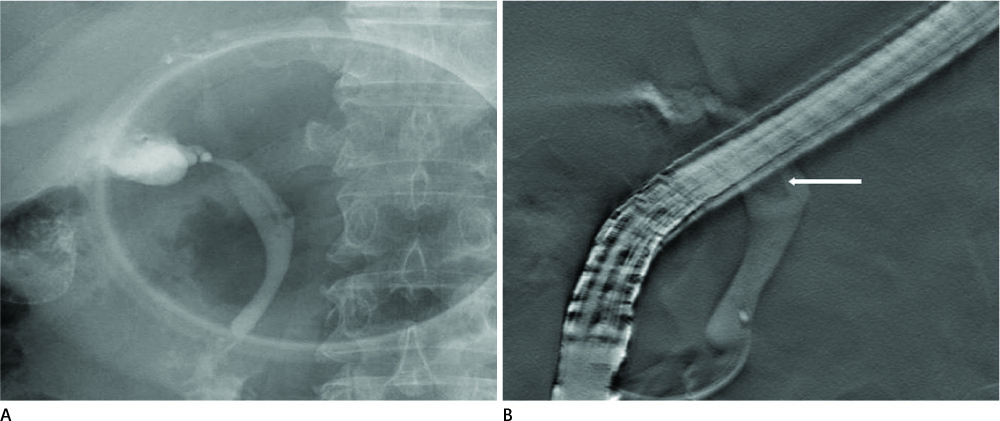
Fig. 3 A 70-year-old man with one stone in the proximal CBD. A. On ERCP image, no definite CBD stone is visualized. B. Digital tomosynthesis image showing a proximal CBD stone (arrow) with a score of 3 because the upper margin of the CBD stone is obscured. Note.-CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography

Fig. 4 A 66-year-old man with two proximal CBD stones. A. ERCP image obtained after injection of contrast material showing 2 CBD stones (arrows) which are considered to have a score of 2 (upper stone) and 3 (lower stone). B. Digital tomosynthesis image showing 2 CBD stones (arrows) more clearly compared with the visualization in (A), considered as score to have a 5 for both stones. Note.-CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography

Fig. 5 A 74-year-old woman with a CBD stone. A. ERCP image clearly showing a CBD stone (arrow) with a score of 5. B. Digital tomosynthesis image showing the presence of a stone (arrow) in the proximal CBD with blurring of the margin, considered to have a score of 4. Note.-CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography
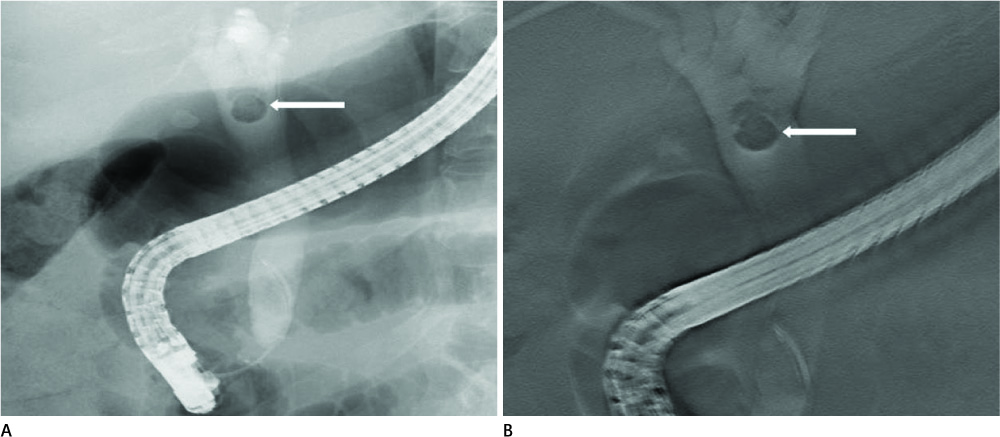
Fig. 6 A 47-year-old woman with a CBD stone. CBD stone (arrow) clearly seen on both the ERCP image (A) and digital tomosynthesis image (B) with a score of 5. Note.-CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography
Reference
-
1. Dobbins JT 3rd, Godfrey DJ. Digital x-ray tomosynthesis: current state of the art and clinical potential. Phys Med Biol. 2003; 48:R65–R106.2. Vikgren J, Zachrisson S, Svalkvist A, Johnsson AA, Boijsen M, Flinck A, et al. Comparison of chest tomosynthesis and chest radiography for detection of pulmonary nodules: human observer study of clinical cases. Radiology. 2008; 249:1034–1041.3. Tingberg A. X-ray tomosynthesis: a review of its use for breast and chest imaging. Radiat Prot Dosimetry. 2010; 139:100–107.4. Dobbins JT 3rd, McAdams HP. Chest tomosynthesis: technical principles and clinical update. Eur J Radiol. 2009; 72:244–251.5. Dobbins JT 3rd, McAdams HP, Godfrey DJ, Li CM. Digital tomosynthesis of the chest. J Thorac Imaging. 2008; 23:86–92.6. Pasanen P, Partanen K, Pikkarainen P, Alhava E, Pirinen A, Janatuinen E. Ultrasonography, CT, and ERCP in the diagnosis of choledochal stones. Acta Radiol. 1992; 33:53–56.7. Pickuth D, Spielmann RP. Detection of choledocholithiasis: comparison of unenhanced spiral CT, US, and ERCP. Hepatogastroenterology. 2000; 47:1514–1517.8. Rickes S, Treiber G, Mönkemüller K, Peitz U, Csepregi A, Kahl S, et al. Impact of the operator's experience on value of high-resolution transabdominal ultrasound in the diagnosis of choledocholithiasis: a prospective comparison using endoscopic retrograde cholangiography as the gold standard. Scand J Gastroenterol. 2006; 41:838–843.9. Stott MA, Farrands PA, Guyer PB, Dewbury KC, Browning JJ, Sutton R. Ultrasound of the common bile duct in patients undergoing cholecystectomy. J Clin Ultrasound. 1991; 19:73–76.10. Kondo S, Isayama H, Akahane M, Toda N, Sasahira N, Nakai Y, et al. Detection of common bile duct stones: comparison between endoscopic ultrasonography, magnetic resonance cholangiography, and helical-computed-tomographic cholangiography. Eur J Radiol. 2005; 54:271–275.11. Breen DJ, Nicholson AA. The clinical utility of spiral CT cholangiography. Clin Radiol. 2000; 55:733–739.12. Persson A, Dahlström N, Smedby O, Brismar TB. Three-dimensional drip infusion CT cholangiography in patients with suspected obstructive biliary disease: a retrospective analysis of feasibility and adverse reaction to contrast material. BMC Med Imaging. 2006; 6:1.13. Nilsson U. Adverse reactions to iotroxate at intravenous cholangiography. A prospective clinical investigation and review of the literature. Acta Radiol. 1987; 28:571–557.14. Griffin N, Wastle ML, Dunn WK, Ryder SD, Beckingham IJ. Magnetic resonance cholangiopancreatography versus endoscopic retrograde cholangiopancreatography in the diagnosis of choledocholithiasis. Eur J Gastroenterol Hepatol. 2003; 15:809–813.15. Kim TK, Kim BS, Kim JH, Ha HK, Kim PN, Kim AY, et al. Diagnosis of intrahepatic stones: superiority of MR cholangiopancreatography over endoscopic retrograde cholangiopancreatography. AJR Am J Roentgenol. 2002; 179:429–434.16. Stiris MG, Tennøe B, Aadland E, Lunde OC. MR cholangiopancreaticography and endoscopic retrograde cholangiopancreaticography in patients with suspected common bile duct stones. Acta Radiol. 2000; 41:269–272.17. Kats J, Kraai M, Dijkstra AJ, Koster K, Ter Borg F, Hazenberg HJ, et al. Magnetic resonance cholangiopancreaticography as a diagnostic tool for common bile duct stones: a comparison with ERCP and clinical follow-up. Dig Surg. 2003; 20:32–37.18. Kessler RE, Falkenstein DB, Clemett AR, Zimmon DS. Indications, clinical value and complications of endoscopic retrograde cholangiopancreatography. Surg Gynecol Obstet. 1976; 142:865–870.19. Silviera ML, Seamon MJ, Porshinsky B, Prosciak MP, Doraiswamy VA, Wang CF, et al. Complications related to endoscopic retrograde cholangiopancreatography: a comprehensive clinical review. J Gastrointestin Liver Dis. 2009; 18:73–82.20. Rieger R, Wayand W. Yield of prospective, noninvasive evaluation of the common bile duct combined with selective ERCP/sphincterotomy in 1390 consecutive laparoscopic cholecystectomy patients. Gastrointest Endosc. 1995; 42:6–12.21. Vitale GC, Larson GM, Wieman TJ, Cheadle WG, Miller FB. The use of ERCP in the management of common bile duct stones in patients undergoing laparoscopic cholecystectomy. Surg Endosc. 1993; 7:9–11.22. Cotton PB. Endoscopic retrograde cholangiopancreatography and laparoscopic cholecystectomy. Am J Surg. 1993; 165:474–478.23. Shiozawa S, Kim DH, Usui T, Tsuchiya A, Masuda T, Inose S, et al. Indication of endoscopic retrograde cholangiography by noninvasive predictive factors of common bile duct stones before laparoscopic cholecystectomy: a prospective clinical study. Surg Laparosc Endosc Percutan Tech. 2011; 21:28–32.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Concurrent Yellow-to-white and Black Extrahepatic Bile Duct Stones
- The Endoscopic Management of Common Bile Duct Stones
- Cholelithiasis Fortunately Removed by Endoscopic Retrograde Cholangiopancreatography
- Ultrasonographic findings of intrahepatic bile duct stone
- A Common Bile Duct Web in Association with Bile Duct Stone Treated with Balloon Dilatation
