Imaging Findings of Liposuction with an Emphasis on Postsurgical Complications
- Affiliations
-
- 1Department of Emergency Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul 06273, Korea.
- 2Department of Radiology, Severance Hospital, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 03722, Korea. yelv@yuhs.ac
- KMID: 2344273
- DOI: http://doi.org/10.3348/kjr.2015.16.6.1197
Abstract
- Liposuction is one of the most frequently performed cosmetic surgeries worldwide for reshaping the body contour. Although liposuction is minimally invasive and relatively safe, it is a surgical procedure, and it carries the risk of major and minor complications. These complications vary from postoperative nausea to life-threatening events. Common complications include infection, abdominal wall injury, bowel herniation, bleeding, haematoma, seroma, and lymphoedema. Life-threatening complications such as necrotizing fasciitis, deep vein thrombosis, and pulmonary embolism have also been reported. In this paper, we provide a brief introduction to liposuction with the related anatomy and present computed tomography and ultrasonography findings of a wide spectrum of postoperative complications associated with liposuction.
Keyword
MeSH Terms
Figure
-

Fig. 1 Illustration of liposuction surgery. Blunt cannula is inserted through small incisions to aspirate fat from subcutaneous layer. Aspirated fat is transferred to suction pump through transparent tube. Operator can know amount of fat aspirated and when to end liposuction by checking amount collected in suction pump.
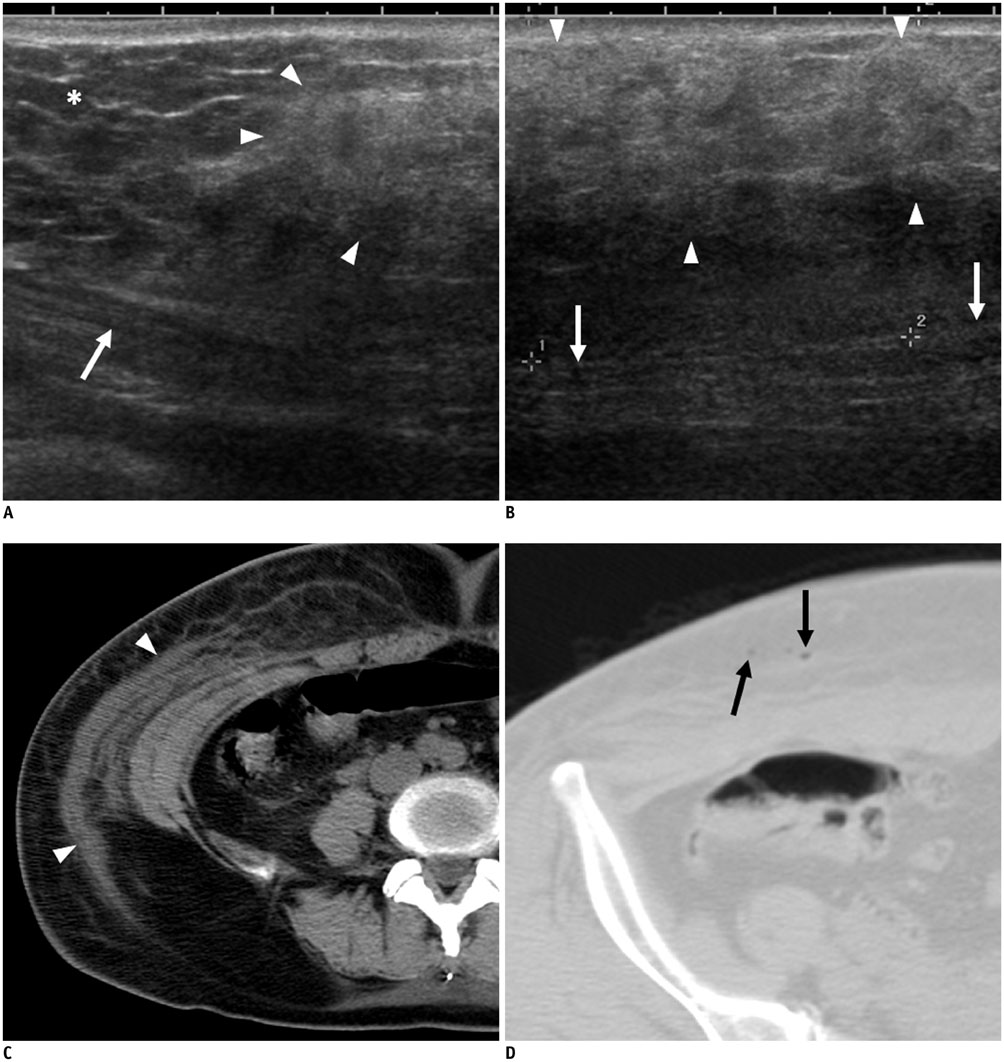
Fig. 2 53-year-old woman who underwent liposuction 3 days previously. She had no symptoms at liposuction site or abdominal wall. A, B. On ultrasonography, heterogeneous hyperechoic area (arrowheads) compared with adjacent normal fat (asterisk) is seen in subcutaneous layer of abdominal wall. Abdominal muscle is seen below lesion (arrows). C. On non-contrast axial CT image, infiltrative lesion with fluid collection or lymphoedema is seen in subcutaneous area (arrowheads). D. Subcutaneous emphysema (arrows) is also seen in subcutaneous layer.
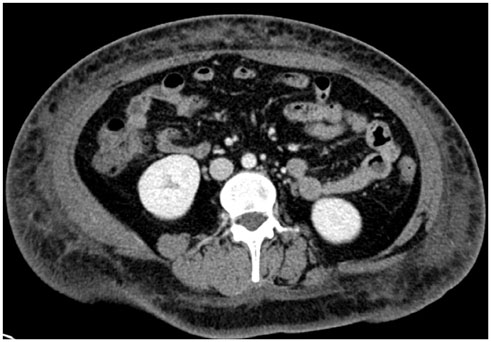
Fig. 3 36-year-old woman presented with persisting fever for 4 days after liposuction. On portal venous-phase CT image, diffuse fat infiltration is seen in subcutaneous layer of body along with suspicious skin thickening. She was diagnosed with cellulitis at liposuction site and treated with intravenous antibiotics after admission.

Fig. 4 36-year-old woman who had received liposuction 2 days before presented with abdominal pain and shock. Her blood pressure was 70 mm Hg systolic and 50 mm Hg diastolic. A. On non-contrast CT image, massive subcutaneous emphysema is seen (arrowheads). At abdominal wall incision, and staining from faecal material is seen at subcutaneous fat layer. B. During exploratory laparotomy, perforation site was detected at ileum. After resection of small bowel and massive peritoneal irrigation, retention suture was made at muscle layer. Subcutaneous fat layer and skin were not closed so that infected material could be effectively drained. C. On photograph taken during surgery, colour changes to rectus sheath are seen, which were likely attributable to inflammation (asterisk). In spite of immediate and intensive care, she died 4 days later.
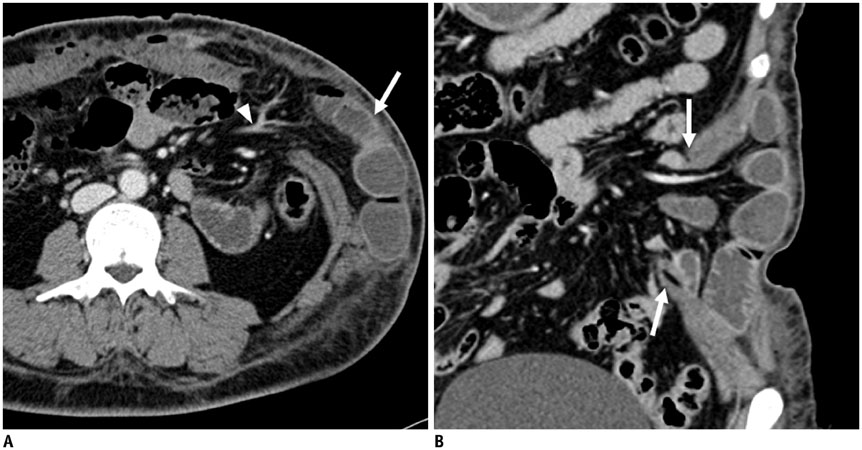
Fig. 5 39-year-old woman presented with abdominal pain and left upper quadrant bulging during liposuction at local clinic. A. Portal venous-phase axial CT images show ventral herniation of small bowel (arrow) with mesentery and associated vessels (arrowhead). Perfusion of bowel wall was preserved. B. On coronal image, full-thickness defects of abdominal wall are seen (arrows). Diagnostic laparoscopy was performed, and reduction of herniated small bowel and layer by layer closure of abdominal wall were performed.
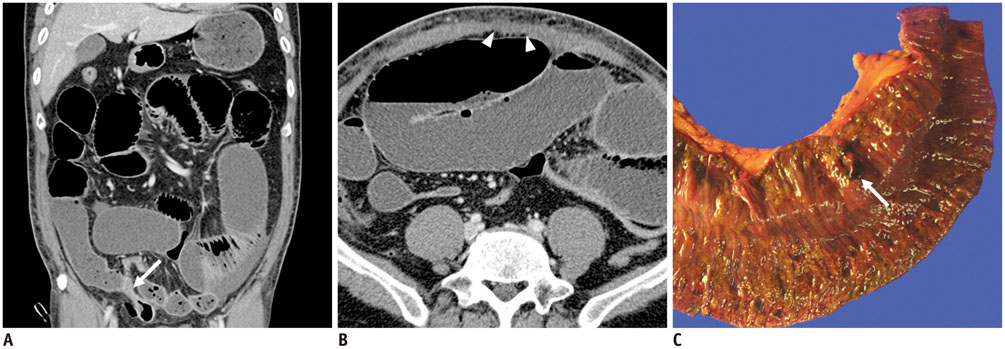
Fig. 6 47-year-old man presented with abdominal distension for 5 days and dyspnoea for 2 days. He had undergone liposuction 5 days previously at local clinic. A. On portal venous-phase coronal CT image, abrupt luminal narrowing of small bowel lumen (arrow) is seen. B. Proximal small bowel was diffusely dilated. Focal defect in rectus muscle (arrowheads) was also detected. On diagnostic laparotomy, perfusion was decreased in distal small bowel loop, and segmental resection of ischemic bowel loop was performed. C. Small perforation site was detected, as seen, at resected small bowel loop (arrow). There were also defects in rectus muscle, in sheath below umbilicus, and at liposuction site. Primary repair of these defects was performed during surgery. Despite undergoing emergency operation, patient did not recover from sepsis and died from multi-organ failure.
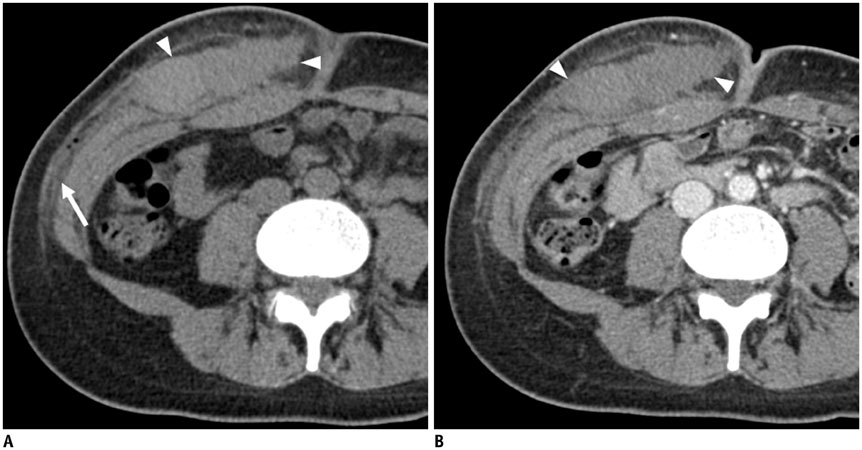
Fig. 7 34-year-old woman who had received liposuction few hours previously presented with swelling and pain in right lower abdominal wall. A. On non-contrast CT image, high-attenuating mass-like lesion is seen in subcutaneous layer of right abdominal wall (arrowheads). Fat infiltration is also seen in subcutaneous layer (arrow). B. On contrast-enhanced CT image, mass-like lesion (arrowheads) does not show enhancement. Contrast media extravasation was also not detected within lesion. She was diagnosed with haematoma without active bleeding in subcutaneous layer of right abdominal wall.
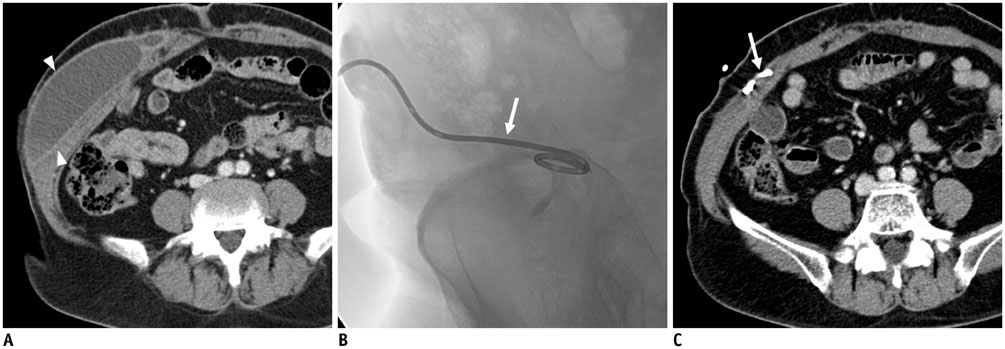
Fig. 8 64-year-old woman presented with abdominal pain and right abdominal wall bulging after liposuction. A. On axial portal venous-phase CT images, loculated fluid collection was noted in right lower abdominal wall (arrowheads). B. Fluoroscopy-guided pigtail catheter (arrow) insertion was performed. C. On follow-up CT, compete drainage of fluid collection is observed. Inserted catheter, which was located within fluid collection, is visible (arrow).
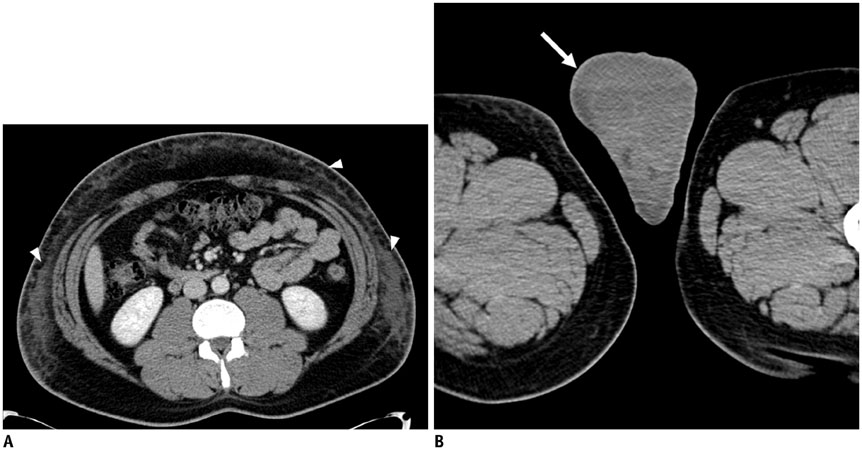
Fig. 9 36-year-old man who had undergone liposuction 3 days previously presented with scrotal swelling that had persisted for 2 days. A. On portal venous-phase CT image, diffuse infiltration, possibly caused by liposuction, is seen (arrowheads). B. On axial CT images of lower pelvis, diffuse subcutaneous oedema (arrow) is noted in scrotum. He was diagnosed with lymphoedema of scrotum caused by liposuction.

Fig. 10 43-year-old woman presented with dyspnoea and dizziness. She had undergone liposuction at trunk and both thighs 2 days previously. A. On parasternal short axis view of emergency portable echocardiography, mild pulmonary hypertension (D shape of left ventricle [LV], estimated right ventricular [RV] systolic pressure = 45 mm Hg) was suspected. B. On contrast-enhanced axial CT image, filling defects are seen in both pulmonary arteries (arrows), suggesting pulmonary embolism. She underwent thrombolytic therapy using heparin and tissue plasminogen activator. C. On follow-up chest CT 6 months later, pulmonary embolism was found to have completely resolved.

Fig. 11 26-year-old female who had received liposuction few hours before visiting hospital presented with abdominal pain and vomiting. Because BUN and serum creatinine showed increased levels of 35.5 mg/dL (normal range: 7.3-20.5 mg/dL) and 2.6 mg/dL (normal range: 0.49-0.91 mg/dL) on laboratory examination, only non-contrast CT scan was performed. On axial CT image, diffuse subcutaneous emphysema was seen (arrowheads). Both kidneys showed oedematous change without hydronephrosis. Patient was diagnosed with pre-renal acute renal failure. After intravenous administration of fluid, her renal function recovered without sequelae.
Reference
-
1. Lehnhardt M, Homann HH, Daigeler A, Hauser J, Palka P, Steinau HU. Major and lethal complications of liposuction: a review of 72 cases in Germany between 1998 and 2002. Plast Reconstr Surg. 2008; 121:396e–403e.2. Kim YH, Cha SM, Naidu S, Hwang WJ. Analysis of postoperative complications for superficial liposuction: a review of 2398 cases. Plast Reconstr Surg. 2011; 127:863–871.3. Stephan PJ, Kenkel JM. Updates and advances in liposuction. Aesthet Surg J. 2010; 30:83–97. quiz 98-1004. Grazer FM, de Jong RH. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast Reconstr Surg. 2000; 105:436–446. discussion 447-4485. Frank SJ, Flusberg M, Friedman S, Swinburne N, Sternschein M, Wolf EL, et al. CT appearance of common cosmetic and reconstructive surgical procedures and their complications. Clin Radiol. 2013; 68:e72–e78.6. Shridharani SM, Broyles JM, Matarasso A. Liposuction devices: technology update. Med Devices (Auckl). 2014; 7:241–251.7. Lipoadvisor. Lipotite/BodyTite. lipoadvisor.com Web site. Accessed June 3, 2015. http://www.lipoadvisor.com/lipotite-bodytite/.8. Matarasso A, Levine SM. Evidence-based medicine: liposuction. Plast Reconstr Surg. 2013; 132:1697–1705.9. Sterodimas A, Boriani F, Magarakis E, Nicaretta B, Pereira LH, Illouz YG. Thirtyfour years of liposuction: past, present and future. Eur Rev Med Pharmacol Sci. 2012; 16:393–406.10. Rozen WM, Ashton MW, Taylor GI. Reviewing the vascular supply of the anterior abdominal wall: redefining anatomy for increasingly refined surgery. Clin Anat. 2008; 21:89–98.11. Grevious MA, Cohen M, Shah SR, Rodriguez P. Structural and functional anatomy of the abdominal wall. Clin Plast Surg. 2006; 33:169–179. v12. Fayad LM, Carrino JA, Fishman EK. Musculoskeletal infection: role of CT in the emergency department. Radiographics. 2007; 27:1723–1736.13. U.S. Food and Drug Administration. Liposuction: What are the risks or complications? FDA.com Web site. Last updated January 16, 2015. Accessed June 3, 2015. http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/SurgeryandLifeSupport/Liposuction/ucm256139.htm.14. Lim H, Kim HJ, Cho YS. Active bleeding in abdominal wall developing after liposuction. Emerg Med J. 2008; 25:814.15. Kwak JY, Lee SH, Park HL, Kim JY, Kim SE, Kim EK. Sonographic findings in complications of cosmetic breast augmentation with autologous fat obtained by liposuction. J Clin Ultrasound. 2004; 32:299–301.16. Frank SJ, Flusberg M, Friedman S, Sternschein M, Wolf EL, Stein MW. Aesthetic surgery of the buttocks: imaging appearance. Skeletal Radiol. 2014; 43:133–139.17. Shin SU, Lee W, Park EA, Shin CI, Chung JW, Park JH. Comparison of characteristic CT findings of lymphedema, cellulitis, and generalized edema in lower leg swelling. Int J Cardiovasc Imaging. 2013; 29:Suppl 2. 135–143.18. Chung YE, Kim YE, Park I, You JS. Subcutaneous emphysema after carbon dioxide injection. J Emerg Med. 2014; 47:e89–e90.19. Hakkarainen TW, Kopari NM, Pham TN, Evans HL. Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes. Curr Probl Surg. 2014; 51:344–362.20. Chaudhry AA, Baker KS, Gould ES, Gupta R. Necrotizing fasciitis and its mimics: what radiologists need to know. AJR Am J Roentgenol. 2015; 204:128–139.21. Dixit VV, Wagh MS. Unfavourable outcomes of liposuction and their management. Indian J Plast Surg. 2013; 46:377–392.22. Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of venous thromboembolism. Chest. 2001; 119:1 Suppl. 132S–175S.23. Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008; 133:6 Suppl. 381S–453S.24. Esmon CT. Basic mechanisms and pathogenesis of venous thrombosis. Blood Rev. 2009; 23:225–229.25. Han D, Lee KS, Franquet T, Müller NL, Kim TS, Kim H, et al. Thrombotic and nonthrombotic pulmonary arterial embolism: spectrum of imaging findings. Radiographics. 2003; 23:1521–1539.26. Cantarelli J, Godoy MF. Safe limits for aspirate volume under wet liposuction. Obes Surg. 2009; 19:1642–1645.27. Di Martino M, Nahas FX, Barbosa MV, Montecinos Ayaviri NA, Kimura AK, Barella SM, et al. Seroma in lipoabdominoplasty and abdominoplasty: a comparative study using ultrasound. Plast Reconstr Surg. 2010; 126:1742–1751.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of an abscess after massive autologous fat transplantation for breast augmentation with real-time ultrasonography-guided liposuction
- Power-Assisted Liposuction and Periareolar Pull-Out Technique for the Treatment of Gynecomastia
- Median Nerve Injury after Liposuction of Upper Arm
- Experiences of Seroma after Lipoabdominoplasty
- Using of a Straw as Liposuction Protector at the Treatment of Osmidrosis
