Macular Hole Formation in Rhegmatogenous Retinal Detachment after Scleral Buckling
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Ophthalmology, Pusan National University Hospital, Busan, Korea. jlee@pusan.ac.kr
- 4Medical institute, Pusan National University School of Medicine, Busan, Korea.
- KMID: 2344259
- DOI: http://doi.org/10.3341/kjo.2014.28.5.364
Abstract
- PURPOSE
To describe early macular hole (MH) development in rhegmatogenous retinal detachment (RRD) after scleral buckling (SB) based on optical coherence tomography (OCT) findings.
METHODS
The medical records and spectral domain OCT images of patients in whom MH developed after RRD repair were evaluated retrospectively.
RESULTS
A postoperative MH was detected in five eyes that underwent SB during a 6-year period. All had fovea-off RRD without MH at the time of surgery. OCT showed partial loss of the inner retina with a preserved photoreceptor layer in early postoperative days. On average, 7 days (range,5 to 8 days) after surgery, outer retinal tissues disappeared, resulting in the full-thickness MH.
CONCLUSIONS
Serial OCT findings revealed that partial-thickness lamellar holes progressed to full-thickness MHs, which were formed by the degeneration of the outer retina in eyes with preceding loss of the glial cone in the fovea.
MeSH Terms
Figure
-
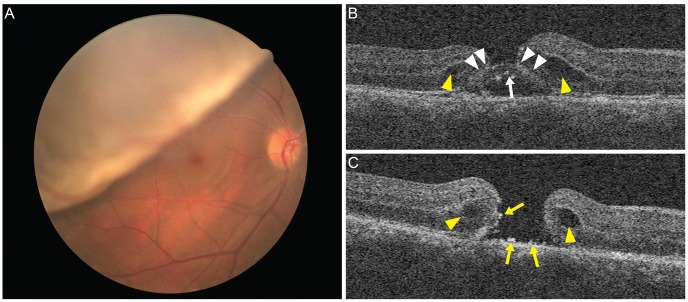
Fig. 1 Fundus photograph and optical coherence tomography obtained from patient 1. (A) Fundus photograph showed superior bullous rhegmatogenous retinal detachment with fovea-off. (B) Optical coherence tomography scan on the second postoperative day. Outer retinal tissue (arrow) and residual fluid were seen on the fovea. Retinal cleavage (arrowhead) at the level of the external limiting membrane, perifoveal elevation, and intraretinal edema (yellow arrowhead) were detected. (C) Day 8. The outer retinal tissue of the fovea was gone and a full-thickness macular hole developed. Fine precipitates and sheddings (yellow arrows) were found on the base and wall of the hole. An intraretinal cyst (yellow arrowhead) remained.
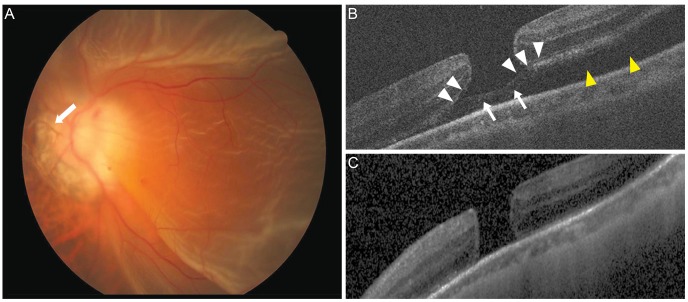
Fig. 2 Fundus photograph and optical coherence tomography obtained from patient 2. (A) Fundus photograph showed fovea-off rhegmatogenous retinal detachment and myopic crescent. Weiss ring (arrow) was visible. (B) Optical coherence tomography scan on the second postoperative day. Outer retinal tissue (arrow) of the fovea with low signal, and residual fluid (yellow arrowhead) at the temporal macula were seen. Retinal cleavage (arrowhead) also was detected at the level of the external limiting membrane. (C) Day 5. Subretinal fluid and retinal tissue disappeared, which resulted in a full-thickness macular hole with a flat edge.
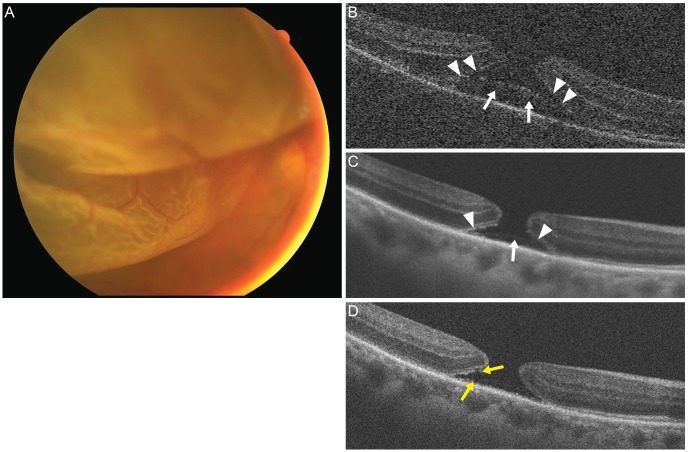
Fig. 3 Fundus photograph and optical coherence tomography obtained from patient 3. (A) Fundus photograph showed bullous rhegmatogenous retinal detachment with fovea-off. (B) Optical coherence tomography scan on the first postoperative day. The perifovea was edematous. Outer retinal tissue (arrow) of the fovea with a low signal, and cleavage (arrowheads) at the level of external limiting membrane were detected. (C) Day 7. The outer retinal tissue of the fovea (arrow) was more diminished, and perifoveal elevation decreased. The cleavage (arrowheads) was remained. (D) Day 10. The outer retinal tissue disappeared, and a full-thickness macular hole with fine precipitates and sheddings (yellow arrows) on the base and wall of the hole were detected.
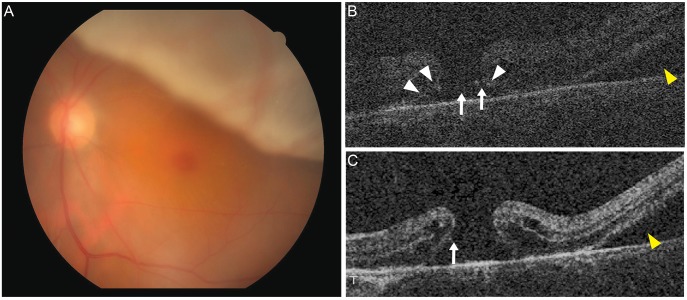
Fig. 4 Fundus photograph and optical coherence tomography obtained from patient 4. (A) Fundus photograph showed fovea-off rhegmatogenous retinal detachment. (B) Postoperative day 8. Retinal cleavage (arrowhead) and outer retina tissue or precipitate-like materials (arrow) were detected with residual fluids (yellow arrowhead). (C) Postoperative day 15. Retinal tissues diminished further at the fovea, forming a full-thickness macular hole with perifoveal edema. Precipitate was seen on the lateral wall of hole (arrow). Subretinal fluid (yellow arrowhead) was remained.
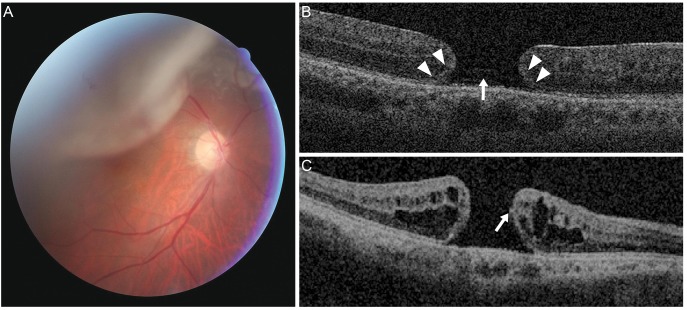
Fig. 5 Fundus photograph and optical coherence tomography obtained from patient 5. (A) Fundus photograph shows superior bullous rhegmatogenous retinal detachment with fovea-off. (B) Postoperative day 6. Retinal cleavage (arrowhead) and foveal tissues (arrow), which looked like a macular hole with a flat edge, were seen faintly. (C) Twenty-five months after rhegmatogenous retinal detachment repair, a full-thickness macular hole and perifoveal edema were found. Precipitate-like material was seen on the lateral wall of the hole (arrow).
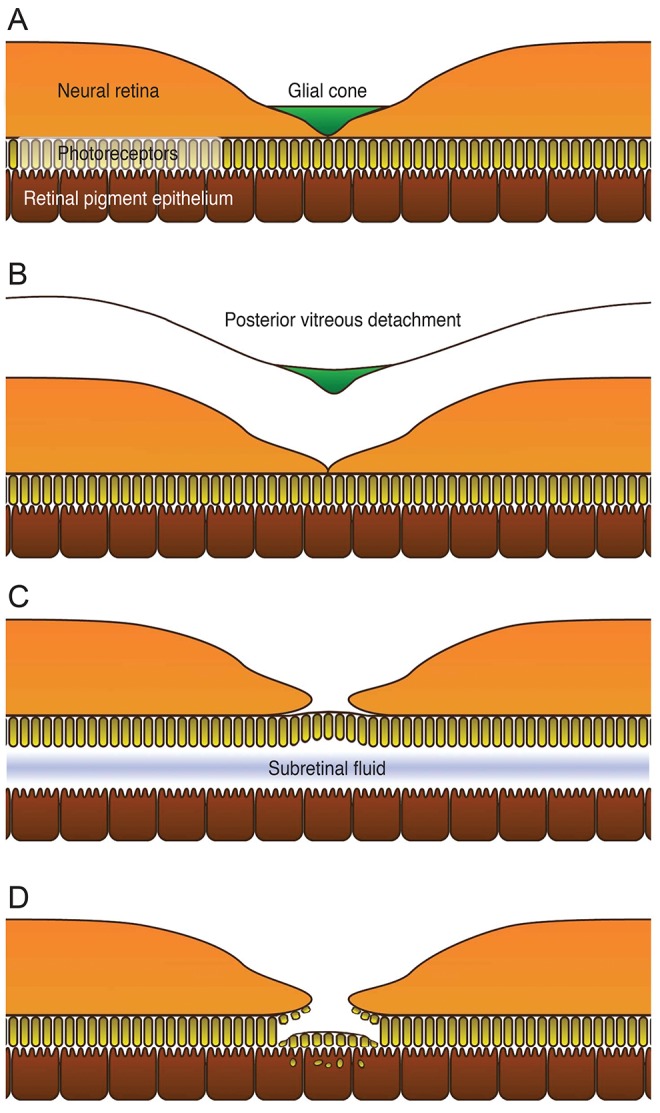
Fig. 6 Schematic representation of macular hole formation in fovea-off rhegmatogenous retinal detachment after repair. (A) Before posterior vitreous detachment, the glial cone is intact and supports the structure of the fovea. (B) The glial cone is removed during posterior vitreous detachment, and the fovea is compromised. (C) Fovea-off rhegmatogenous retinal detachment induces outer retinal ischemia due to deprivation of diffusion from choroidal circulation. The external limit ing membrane provides temporary stability for the separated photoreceptors. (D) Finally, despite reattachment of the retina, degeneration of photoreceptors continues, resulting from the absorption of subretinal fluid and phagocytosis of the degenerated photoreceptors to accelerate development of a full-thickness macular hole.
Reference
-
1. Gass JD. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995; 119:752–759. PMID: 7785690.
Article2. Gaudric A, Haouchine B, Massin P, et al. Macular hole formation: new data provided by optical coherence tomography. Arch Ophthalmol. 1999; 117:744–751. PMID: 10369584.3. Smiddy WE, Flynn HW Jr. Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004; 137:525–537. PMID: 15013877.
Article4. Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010; 149:371–382. PMID: 20172065.
Article5. Haouchine B, Massin P, Gaudric A. Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology. 2001; 108:15–22. PMID: 11150257.6. Ito Y, Terasaki H, Suzuki T, et al. Mapping posterior vitreous detachment by optical coherence tomography in eyes with idiopathic macular hole. Am J Ophthalmol. 2003; 135:351–355. PMID: 12614753.
Article7. Takahashi A, Nagaoka T, Ishiko S, et al. Foveal anatomic changes in a progressing stage 1 macular hole documented by spectral-domain optical coherence tomography. Ophthalmology. 2010; 117:806–810. PMID: 20132987.
Article8. Takahashi A, Yoshida A, Nagaoka T, et al. Idiopathic full-thickness macular holes and the vitreomacular interface: a high-resolution spectral-domain optical coherence tomography study. Am J Ophthalmol. 2012; 154:881–892. PMID: 22958859.
Article9. Yeh PT, Chen TC, Yang CH, et al. Formation of idiopathic macular hole-reappraisal. Graefes Arch Clin Exp Ophthalmol. 2010; 248:793–798. PMID: 20127106.
Article10. Brown GC. Macular hole following rhegmatogenous retinal detachment repair. Arch Ophthalmol. 1988; 106:765–766. PMID: 3370002.
Article11. Boscia F, Recchimurzo N, Cardascia N, et al. Macular hole following conventional repair of bullous retinal detachment using air injection (D-ACE procedure). Eur J Ophthalmol. 2004; 14:572–574. PMID: 15638111.
Article12. Moshfeghi AA, Salam GA, Deramo VA, et al. Management of macular holes that develop after retinal detachment repair. Am J Ophthalmol. 2003; 136:895–899. PMID: 14597042.
Article13. Benzerroug M, Genevois O, Siahmed K, et al. Results of surgery on macular holes that develop after rhegmatogenous retinal detachment. Br J Ophthalmol. 2008; 92:217–219. PMID: 18227202.
Article14. Smiddy WE. Atypical presentations of macular holes. Arch Ophthalmol. 1993; 111:626–631. PMID: 8489442.
Article15. Tornambe PE. Macular hole genesis: the hydration theory. Retina. 2003; 23:421–424. PMID: 12824853.16. Smiddy WE. Macular hole formation without vitreofoveal traction. Arch Ophthalmol. 2008; 126:737–738. PMID: 18474794.
Article17. Besirli CG, Johnson MW. Traction-induced foveal damage predisposes eyes with pre-existing posterior vitreous detachment to idiopathic macular hole formation. Eye (Lond). 2012; 26:792–795. PMID: 22388594.
Article18. Yamada E. Some structural features of the fovea centralis in the human retina. Arch Ophthalmol. 1969; 82:151–159. PMID: 4183671.
Article19. Gass JD. Muller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacualr retinoschisis. Arch Ophthalmol. 1999; 117:821–823. PMID: 10369597.20. Tsuboi S, Taki-Noie J, Emi K, Manabe R. Fluid dynamics in eyes with rhegmatogenous retinal detachments. Am J Ophthalmol. 1985; 99:673–676. PMID: 4014391.
Article21. Garcia-Arumi J, Boixadera A, Martinez-Castillo V, et al. Macular holes after rhegmatogenous retinal detachment repair: surgical management and functional outcome. Retina. 2011; 31:1777–1782. PMID: 21606891.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Study of Macular Hole Retinal Detachment Associated with Peripheral Retinal Hole
- Clinical Analysis of Laser Photocoagulation Following Scleral Buckling for the Treatment of Rhegmatogenous Retinal Detachment
- A Case of Retinal Detachment with Equatorial Scleral Staphyloma
- A Case of Retinal Detachment with Equatorial Scleral Staphyloma
- Comparative Analysis of Scleral Buckling With or Without Postoperative Photocoagulation
