Pathological Substratum for a Case of Fulminant Myocarditis Treated with Extracorporeal Membrane Oxygenation and Subsequent Heart Transplantation
- Affiliations
-
- 1Department of Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 2Division of Cardiology, Department of Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. yang.hyun@gmail.com
- 3Department of Pathology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- KMID: 2344166
- DOI: http://doi.org/10.3346/jkms.2015.30.9.1367
Abstract
- Fulminant myocarditis has been defined as the clinical manifestation of cardiac inflammation with rapid-onset heart failure and cardiogenic shock. We report on the case of a 23-yr-old woman with pathology-proven fulminant lymphocytic myocarditis presenting shock with elevated cardiac troponin I and ST segments in V1-2, following sustained ventricular tachycardia and a complete atrioventricular block. About 55 min of intensive cardio-pulmonary resuscitation, with extracorporeal membrane oxygenation support, bridged the patient to orthotopic heart transplantation. The explanted heart revealed diffuse lymphocytic infiltration and myocyte necrosis in all four cardiac chamber walls. Aggressive mechanical circulatory support may be an essential bridge for recovery or even transplantation in patients with fulminant myocarditis with shock.
Keyword
MeSH Terms
Figure
-
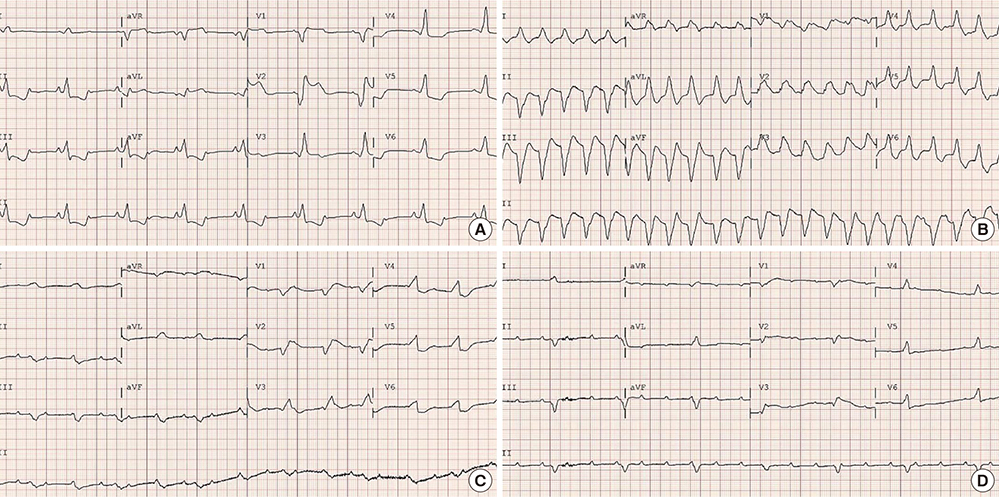
Fig. 1 Electrocardiograms before the orthotopic heart transplantation. (A) In the emergency room there was a 2:1 atrioventricular block with an elevated ST-T segments at V1-2 and reciprocal ST depression in leads II, III, aVF, and V4-6. (B) Before the ECMO support, there was sustained ventricular tachycardia. (C, D) At hospital days 3 and 4, there was a complete atrioventricular block with a progress of low voltage R waves.
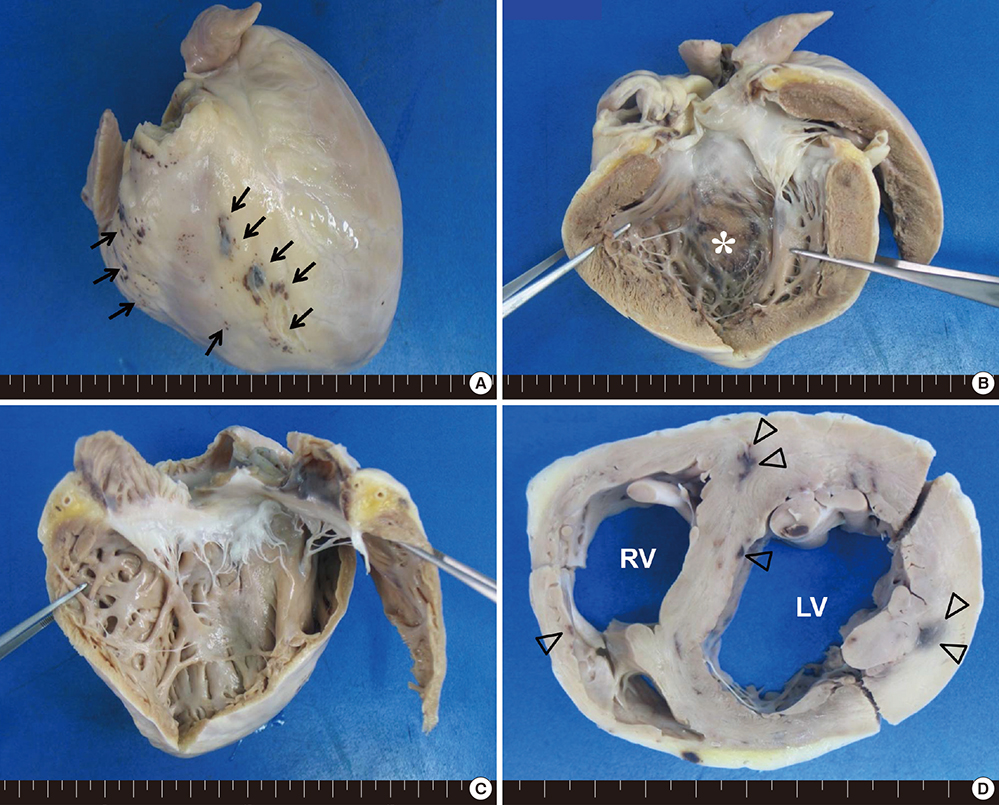
Fig. 2 Gross findings of the explant heart. The heart measured 10.2×7.8×7.2 cm, and weighed 236 grams. (A) On inspection, the external surface shows multiple petechia-like lesions (black arrows). (B) A longitudinal cut section of the left ventricle (LV) endocardium reveals multiple erythematous and dark hemorrhagic spots (white asterisk). (C) The right ventricle (RV) endocardium shows a bright brown and relatively homogeneous appearance. (D) An axial cut section of both ventricles shows multifocal areas of mottling (empty arrowheads).
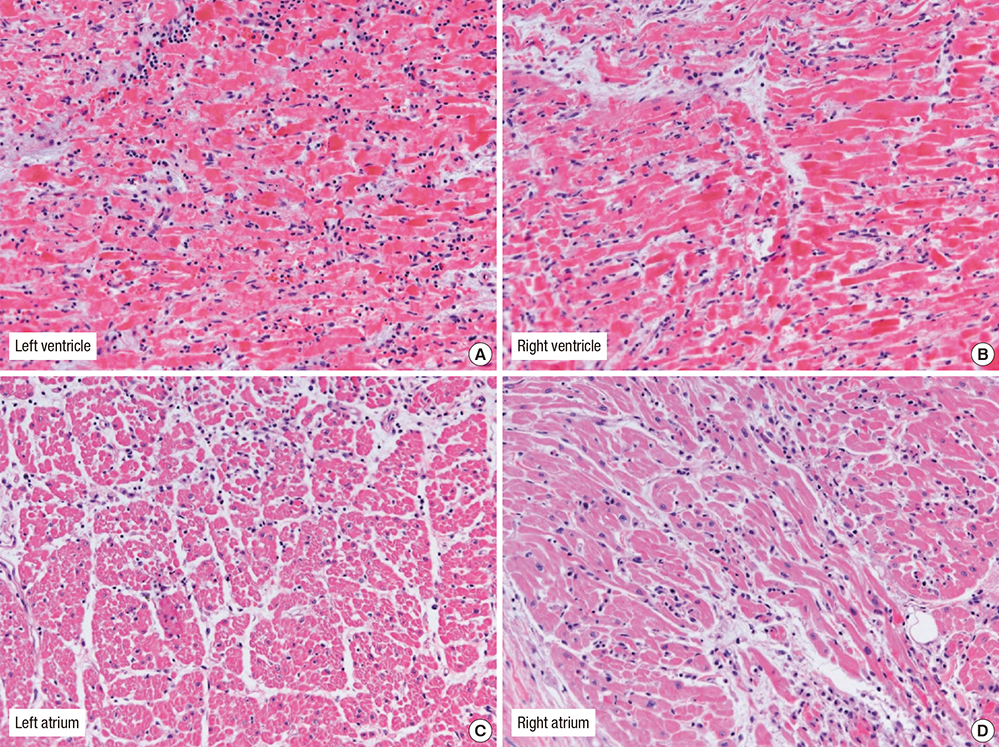
Fig. 3 Histologic findings of the explant heart. (A) Left ventricle, (B) Right ventricle, (C) Left atrium, and (D) Right atrium. Both atrial and ventricular walls show fulminant lymphocytic myocarditis. There are no giant cells or evidence for vasculitis or granulomas (H&E stain ×200).
Reference
-
1. Grinda JM, Chevalier P, D'Attellis N, Bricourt MO, Berrebi A, Guibourt P, Fabiani JN, Deloche A. Fulminant myocarditis in adults and children: bi-ventricular assist device for recovery. Eur J Cardiothorac Surg. 2004; 26:1169–1173.2. Mody KP, Takayama H, Landes E, Yuzefpolskaya M, Colombo PC, Naka Y, Jorde UP, Uriel N. Acute mechanical circulatory support for fulminant myocarditis complicated by cardiogenic shock. J Cardiovasc Transl Res. 2014; 7:156–164.3. Nahum E, Dagan O, Lev A, Shukrun G, Amir G, Frenkel G, Katz J, Michel B, Birk E. Favorable outcome of pediatric fulminant myocarditis supported by extracorporeal membranous oxygenation. Pediatr Cardiol. 2010; 31:1059–1063.4. Ghelani SJ, Spaeder MC, Pastor W, Spurney CF, Klugman D. Demographics, trends, and outcomes in pediatric acute myocarditis in the United States, 2006 to 2011. Circ Cardiovasc Qual Outcomes. 2012; 5:622–627.5. Aretz HT. Myocarditis: the Dallas criteria. Hum Pathol. 1987; 18:619–624.6. McCarthy RE 3rd, Boehmer JP, Hruban RH, Hutchins GM, Kasper EK, Hare JM, Baughman KL. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000; 342:690–695.7. Wilmot I, Morales DL, Price JF, Rossano JW, Kim JJ, Decker JA, McGarry MC, Denfield SW, Dreyer WJ, Towbin JA, et al. Effectiveness of mechanical circulatory support in children with acute fulminant and persistent myocarditis. J Card Fail. 2011; 17:487–494.8. Mahrholdt H, Goedecke C, Wagner A, Meinhardt G, Athanasiadis A, Vogelsberg H, Fritz P, Klingel K, Kandolf R, Sechtem U. Cardiovascular magnetic resonance assessment of human myocarditis: a comparison to histology and molecular pathology. Circulation. 2004; 109:1250–1258.9. Pankuweit S, Portig I, Eckhardt H, Crombach M, Hufnagel G, Maisch B. Prevalence of viral genome in endomyocardial biopsies from patients with inflammatory heart muscle disease. Herz. 2000; 25:221–226.10. Narula N, McNamara DM. Endomyocardial biopsy and natural history of myocarditis. Heart Fail Clin. 2005; 1:391–406.11. Chen YS, Yu HY, Huang SC, Chiu KM, Lin TY, Lai LP, Lin FY, Wang SS, Chu SH, Ko WJ. Experience and result of extracorporeal membrane oxygenation in treating fulminant myocarditis with shock: what mechanical support should be considered first. J Heart Lung Transplant. 2005; 24:81–87.12. Song SW, Yang HS, Lee S, Youn YN, Yoo KJ. Earlier application of percutaneous cardiopulmonary support rescues patients from severe cardiopulmonary failure using the APACHE III scoring system. J Korean Med Sci. 2009; 24:1064–1070.13. Lieberman EB, Hutchins GM, Herskowitz A, Rose NR, Baughman KL. Clinicopathologic description of myocarditis. J Am Coll Cardiol. 1991; 18:1617–1626.14. Haas GJ. Etiology, evaluation, and management of acute myocarditis. Cardiol Rev. 2001; 9:88–95.15. Freund MW, Kleinveld G, Krediet TG, van Loon AM, Verboon-Maciolek MA. Prognosis for neonates with enterovirus myocarditis. Arch Dis Child Fetal Neonatal Ed. 2010; 95:F206–F212.16. Rupprecht L, Flörchinger B, Schopka S, Schmid C, Philipp A, Lunz D, Müller T, Camboni D. Cardiac decompression on extracorporeal life support: a review and discussion of the literature. ASAIO J. 2013; 59:547–553.17. Adebo OA, Lun KC, Lee CN, Chao TC. Age-related changes in normal Chinese hearts. Chin Med J (Engl). 1994; 107:88–94.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Extracorporeal Membrane Oxygenation (ECMO) for Acute Fulminant Myocarditis
- Giant Cell Myocarditis Manifested as Fulminant Myocarditis
- Two cases of acute fulminant myocarditis supported by extracorporeal membrane oxygenation
- Successfully Treated Acute Fulminant Myocarditis Induced by Ulcerative Colitis with Extracorporeal Life Support and Infliximab
- Life-Threatening Acute Fulminant Myocarditis Following a Coffee Diet Program
