J Korean Ophthalmol Soc.
2013 Dec;54(12):1875-1881.
Diagnostic Criteria of Pattern VEP in Adult Monocular Amblyopic Patients
- Affiliations
-
- 1Department of Ophthalmology, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. Limkh@ewha.ac.kr
Abstract
- PURPOSE
To suggest a diagnostic criteria of pattern visual evoked potential (VEP) in adult monocular amblyopic patients in comparison to normal subjects.
METHODS
The medical records of patients' military service certificates from January 2000 to December 2011 were reviewed. The parameters of pattern VEP were analyzed by comparing monocular amblyopic patients with normal controls.
RESULTS
This study included 47 monocular amblyopia and 39 normal control patients. All parameters of pattern VEP were statistically significantly different between monocular amblyopic eyes and normal eyes. The cut-off values for diagnosis of adult amblyopia using receiver operating characteristic (ROC) curve were 113.50 msec (P100 latency), 1.05 (ratio of P100 latency), 8.50 msec (interocular difference of P100 latency), and 5.25 microV (interocular difference of P100 amplitude). Cut-off value sensitivities were generally low: (51.1%, 70.2%, 53.2%, and 31.9%, respectively).
CONCLUSIONS
The value of pattern VEP parameters had limitations due to low sensitivity and could be considered as ancillary diagnostic criteria when diagnosing amblyopia.
MeSH Terms
Figure
-
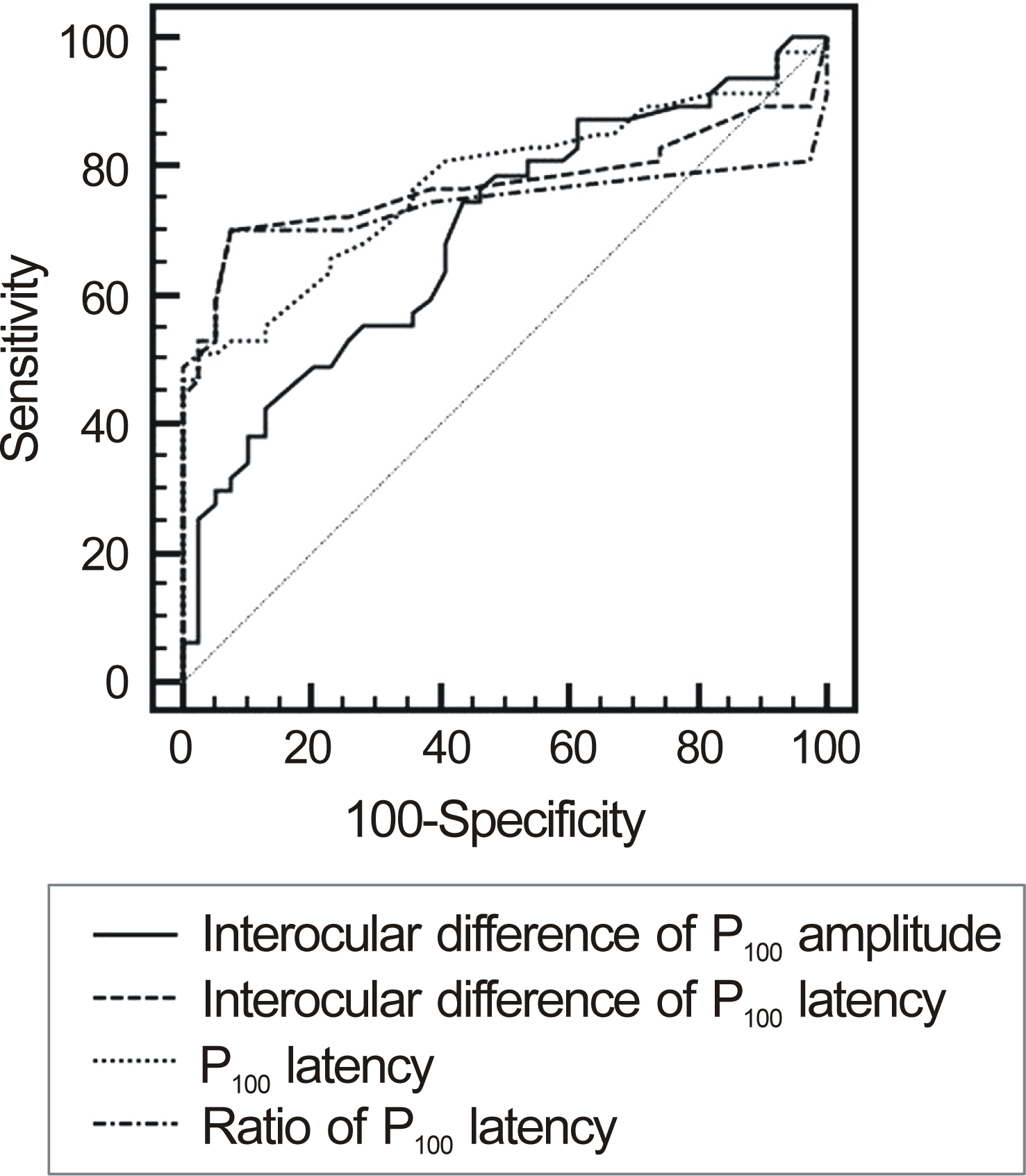
Figure 1. Receiver operating characteristics (ROC) curve of the parameters of visual evoked potential (VEP).
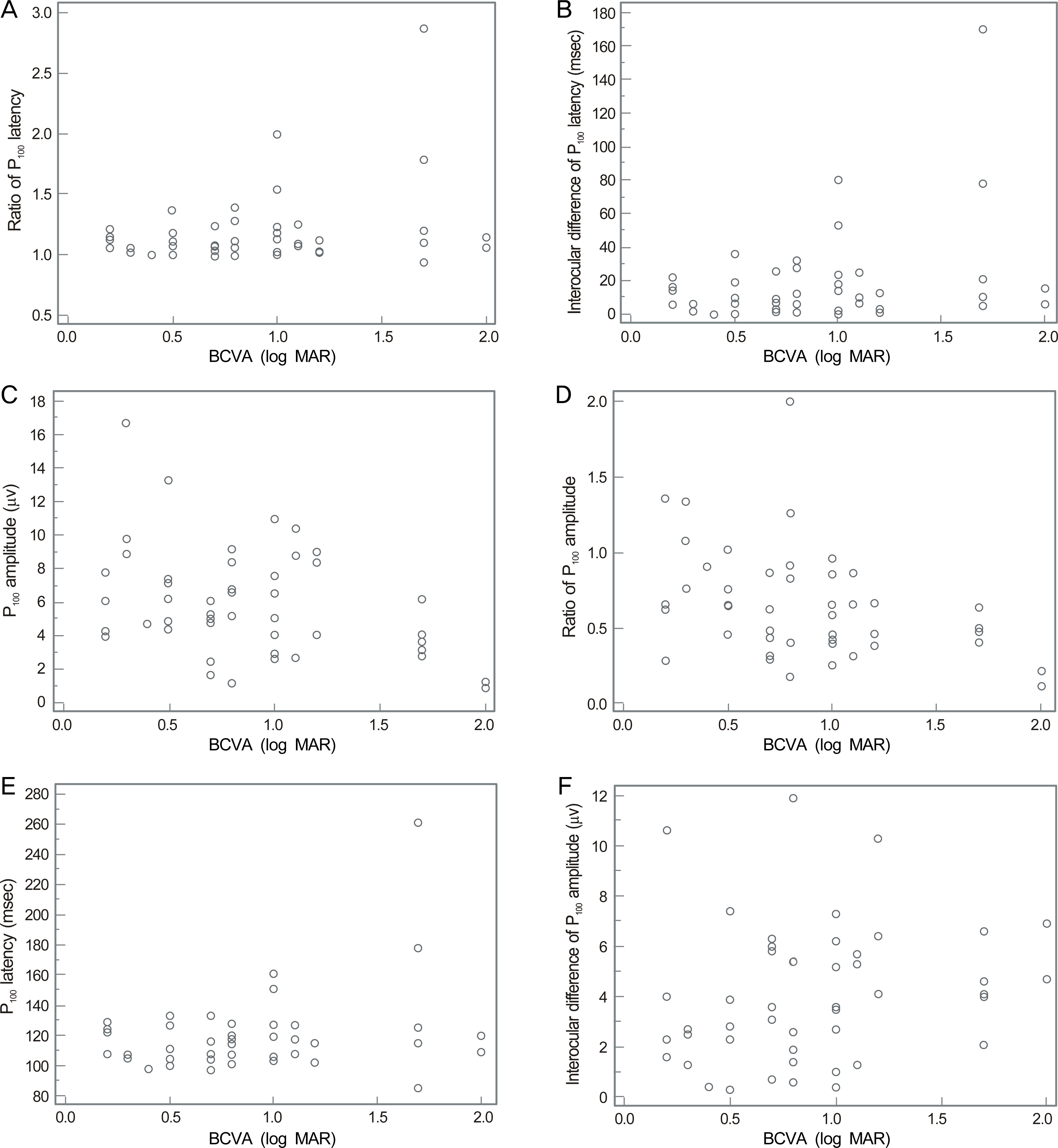
Figure 2. Correlations between visual acuity (log MAR) and Visual evoked potential (VEP) parameters of amblyopic patients. Log MAR and ratio of P100 latency (A) and interocular difference of P100 latency (B) have positive correlation which is statistically significant (p < 0.05). Log MAR and P100 amplitude (C) and ratio of P100 amplitude (D) have negative correlation which is statistically significant (p < 0.05). Log MAR and P100 latency (E) and interocular difference of P100 amplitude (F) have positive correlation which is not statistically significant (p > 0.05). * BCVA = best corrected visual acuity.
Reference
-
References
1. Yoo WS, Park YJ, Yoo JM. Pattern VEP in adult amblyopic pa-tients requested from military service. J Korean Ophthalmol Soc. 2010; 51:1392–7.
Article2. Park HK, Kim MM, Hahn DK. Evaluation of VEP in optic nerve diseases and amblyopia. J Korean Ophthalmol Soc. 1995; 36:1569–73.3. Sokol S, Bloom B. Visually evoked cortical responses of am-blyopes to a spatially alternating stimulus. Invest Ophthalmol. 1973; 12:936–9.4. Szklo M, Nieto FJ. Epidemiology: beyond the basics. 2nd ed.Massachusetts: Jones and Bartlett Learning;2007. p. 319.5. Wanger P, Persson HE. Visually evoked cortical responses to pat-tern reversal stimulation in childhood amblyopia. Acta Ophthalmol. 1980; 58:697–706.6. Park MS, Jin KH, Kim SM. Type of refractive errors and VEP in anisometropic amblyopia. J Korean Ophthalmol Soc. 1990; 31:965–70.7. Odom JV, Bach M, Brigell M. . ISCEV standard for clinical visual evoked potentials (2009 update). Doc Ophthalmol. 2010; 120:111–9.
Article8. Ropper A, Samuels M. Adams and Victor's principles of neurology. 9th ed.NewYork: McGraw Hill Professional;2009. p. 29–31.9. Skuse NF, Burke D, McKeon B. Reproducibility of the visual evoked potential using a light-emitting diode stimulator. J Neurol Neurosurg Psychiatry. 1984; 47:623–9.
Article10. Gurstman BB. Epidemiology kept simple: an introduction to classic and modern epidemiology. 2nd ed.New Jersey: Wiley-Liss;2003. p. 90–1.11. Jin KH, Kwak HW, Kim SM. Effect of occlusion therapy and change of VEP in amblyopia. J Korean Ophthalmol Soc. 1987; 28:1041–5.12. Hoe JW, Kim CW, Kim SM. VEP and pattern ERG in adult amblyopes. J Korean Ophthalmol Soc. 1990; 31:1481–8.13. Young B, Eggenberger E, Kaufman D. Current electrophysiology in ophthalmology: a review. Curr Opin Ophthalmol. 2012; 23:497. 505.14. Sokol S. Visually evoked potentials: Theory, technique and clinical applications. Surv Ophthalmol. 1976; 21:18–44.15. Jeon J, Oh S, Kyung S. Assessment of visual disability using visual evoked potentials. BMC Ophthalmol. 2012; 12:36.
Article16. Yoon GJ, Choi GJ, Ji NC. P100 latency in normal persons by pat-tern reversal VEP and flash VEP. J Korean Ophthalmol Soc. 1996; 37:78–85.17. Sokol S, Moskowitz A, Towle VL. Age-related changes in the la-tency of the visual evoked potential: Influence of check-size. Electroencephalogr Clin Neurophysiol. 1981; 51:559–62.18. Holliday AM, Mcdonald WI, Mushin J. Visual evoked response in diagnosis of multiple sclerosis. Br Med J. 1973; 4:661–4.19. Asselman P, Chadwick DW, Marsden DC. Visual evoked response in diagnosis and management of patients suspected of multiple sclerosis. Brain. 1975; 98:261–82.20. Sokol S. Abnormal evoked potential latencies in amblyopia. Br J Ophthalmol. 1983; 67:310–4.
Article21. Sriram P, Klistorner A, Arvind H, Graham SL. Reproducibility of multifocal VEP latency using different stimulus presentations. Doc Ophthalmol. 2012; 125:43–9.
Article
