Usefulness of Open Ring Guider for Continuous Curvilinear Capsulorrhexis
- Affiliations
-
- 1Department of Ophthalmology, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. ckjoo@catholic.ac.kr
Abstract
- PURPOSE
To compare the size, circularity and repeatability between the conventional manual technique and the open-ring guided continuous curvilinear capsulorrhexis (CCC) technique in cataract surgery.
METHODS
The present study comprised 120 eyes divided into two equal groups. In the first group (group A), CCC was performed using a 5.3-mm open ring-shaped caliper and in the second group (group B), CCC was performed using the conventional manual technique. Photographs were taken after each surgical step (CCC, phacoemulsification, Intraocular lens insertion and corneal stromal hydration). The diameter, area and circularity of the anterior capsule were compared between the two groups.
RESULTS
The anterior capsule diameter was 5.32 +/- 0.26 mm for group A (coefficient of variation 0.049) and 5.14 +/- 0.64 mm for group B (coefficient of variation 0.125); the area was 22.9 +/- 0.71 mm2 for group A (coefficient of variation 0.031) and 21.40 +/- 1.37 mm2 for group B (coefficient of variation 0.064). Circularity was 0.93 +/- 0.24 for group A (coefficient of variation 0.258) and 0.86 +/- 0.78 for group B (coefficient of variation 0.907).
CONCLUSIONS
The open ring-guided CCC technique resulted in an increase of diameter and capsulorrhexis area. This method showed superior circularity and repeatability compared to conventional manual technique and can be useful in cataract surgery.
Keyword
Figure
-

Figure 1. Open Ring Guider for CCC: Inflexible polymethyl methacrylate caliper ring with an internal diameter of 5.3 mm and external diameter of 5.8 mm. It is easy to insert in the eye because of the shape of an open ring (yellow star).
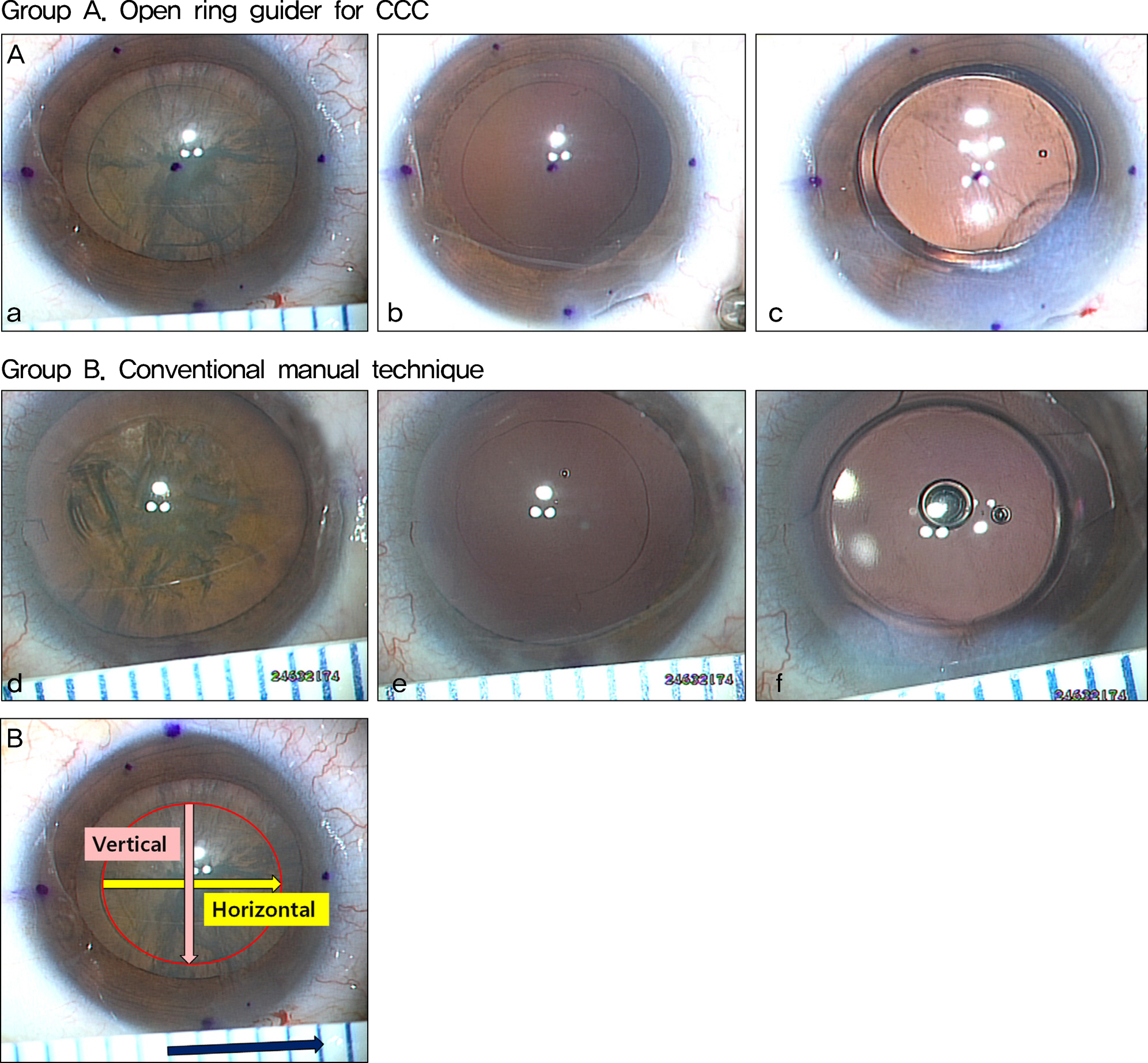
Figure 2. (A) Group A was performed by using a 5.3-mm ORGC (a. after CCC, b. after phacoemulsification, c. after IOL insertion and corneal stromal hydration). Group B was performed by using conventional manual technique (d. after CCC, e. after phacoemulsification, f. after IOL insertion and corneal stromal hydration). (B) Image J's graphic program to measure the diameter, area and circularity of anterior capsule were compared between two groups. (A) Photos were taken after each surgical step. (B) Measuring the diameter, area and circularity of anterior capsule.

Figure 3. Comparison between two groups regarding to the calculated CCC parameters after final step, IOL implantation and corneal stromal hydration stage during cataract surgery.

Figure 4. The coefficient of variation (CV) represents the CCC repeatability that is defined as the ratio of the standard deviation to the mean, it is a helpful statistic in comparing the degree of variation from one data series to the other. It was observed that the lower the CV, the higher the repeatability.
Reference
-
References
1. Gimbel HV, Neuhann T. Development, advantages, and methods of the continuous circular capsulorhexis technique. J Cataract Refract Surg. 1990; 16:31–7.
Article2. Arshinoff S. Mechanics of capsulorhexis. J Cataract Refract Surg. 1992; 18:623–8.
Article3. Eom Y, Kang SY, Kim HM, Song JS. A survey report on cataract surgical experiences during ophthalmology residency in Korea. J Korean Ophthalmol. 2011; 52:429–33.
Article4. Masket S. Postoperative complication of capsulorhexis. J Cataract Refract Surg. 1993; 19:721–4.5. Nishi O, Nishi K. Intraocular lens encapsulation by shrinkage of the capsulorhexis opening. J Cataract Refract Surg. 1993; 19:544–5.
Article6. Aykan U, Bilge AH, Karadayi K, Akin T. The effect of capsulorhexis size on development of posterior capsule opacification: small (4.5 to 5.0 mm) versus large (6.0 to 7.0 mm). Eur J Ophthalmol. 2003; 13:541–5.
Article7. Langwmska-Wosko E, Bronike-kowalik K, Szulborski K. The impact of capsulorhexis diameter, localization and shape on posterior capsule opacification. Med Sci Monit. 2011; 17:CR577–82.
Article8. Budning A, Rosen J. The elastic properties of the lens capsule in capsulorhexis. Am J Ophthalmol. 1991; 112:474–5.
Article9. Thim K, Krag S, Corydon L. . Stretching capacity of capsu- lrhexis and nucleus delivery. J Cataract Refract Surg. 1991; 17:27–31.10. Colvard DM, Dunn SA. Intraocular lens centration with continuous tear capsulotomy. J Cataract Refract Surg. 1990; 16:312–4.
Article11. Gimbel HV, DeBroff BM. Intraocular lens optic capture. J Cataract Refract Surg. 2004; 30:200–6.
Article12. Smith SR, Daynes T, Hinckley M. . The effect of lens edge design versus anterior capsule overlap on posterior capsule opacification. Am J Ophthalmol. 2004; 138:521–6.
Article13. Tassignon MJ, De Groot V, Vrensen GF. Bag-in-the-lens implantation of intraocular lenses. J Cataract Refract Surg. 2002; 28:1182–8.
Article14. Wallace RB 3rd. Capsulotomy diameter mark. J Cataract Refract Surg. 2003; 29:1866–8.
Article15. Kellen RI. Capsulotomy diameter mark. J Cataract Refract Surg. 2004; 30:2031–2.
Article16. Dick HB, Peña-Aceves A, Manns M, Krummenauer F. New technology for sizing the continuous curvilinear capsulorhexis: prospective trial. J Cataract Refract Surg. 2008; 34:1136–44.
Article17. Tassignon MJ, Rozema JJ, Gobin L. Ring-shaped caliper for better anterior capsulorhexis sizing and centration. J Cataract Refract Surg. 2006; 32:1253–5.
Article18. Joo CK, Shin JA, Kim JH. Capsular opening contraction after continuous curvilinear capsulorhexis and intraocular lens implantation. J Cataract Refract Surg. 1996; 22:585–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Capsular Tension Ring on Shape of Capsular Bag, Capsular Opening, and Intraocular Lens
- Clinical Result of Planned posterior Continuous Curvilinear Capsulorrhexis in Adult Cataract patients: 1 year follow-up
- Continuous Curvilinear Capsulorhexis (CCC) Remodeling after CCC Widening with a Nd:YAG Laser
- Clinical Result of Planned Posterior Continuous Curvilinear Capsulorrhexis in Adult Patients
- A Case of Capsule Contraction Syndrome following Continuous Curvilinear Capsulorhexis
