Spontaneous Resolution of Vitreoretinal-Iinterface Disorders
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, The Catholic University of Korea College of Medicine, Seoul, Korea. parkyh@catholic.ac.kr
Abstract
- PURPOSE
To review the mechanisms and clinical patterns of spontaneous resolution of vitreoretinal interface disorders by analyzing cases and available literature on macular hole (MH), vitreoretinal traction (VMT), and epiretinal membrane (ERM).
METHODS
Medical records and optical coherence tomography (OCT) images of patients with spontaneous resolution of MH, VMT, and ERM were reviewed.
RESULTS
Two eyes with VMT, 3 eyes with idiopathic MH, 3 eyes of traumatic MH (including 1 eye with electrical burn), and 2 eyes with ERM showed spontaneous resolution. All eyes except traumatic MH reached a visual acuity better than 0.5 after resolution. All idiopathic MHs achieved anatomic closure in 6 months, and traumatic MHs in 1 month except for the electrical burn case. Seven out of 10 eyes experienced complete posterior vitreous detachment (PVD) during resolution.
CONCLUSIONS
Some cases of vitreoretinal interface disorders can resolve spontaneously with complete PVD or other mechanisms. Indicators predicting spontaneous resolution should be considered in patients with vitreoretinal interface disorder.
Keyword
MeSH Terms
Figure
-

Figure 1. Optical coherence tomography (M-OCT) of idio-pathic vitreomacular traction (VMT) with stage 1a macular hole(MH) (case 2). Initial M-OCT showed VMT with stage 1a MH and subfoveal cysts (A, B). Eight months after the first visit, M-OCT of the same patient revealed closure of macular hole with complete PVD (white arrow) and subfoveal cysts were no longer apparent (C).

Figure 2. Optical coherence tomography (M-OCT) of idio-pathic stage 1a macular hole (MH) (case 4). Initial M-OCT showed stage 1a MH with preexisting complete posterior vit-reous detachment (white arrow at upper right) (A). Four months after the first visit, M-OCT revealed closure of MH with disrupted retinal pigment epithelium and photoreceptor inner/outer segment junction (B). Seven months after the first visit, complete closure of MH was accomplished (C).

Figure 3. Optical coherence tomography (M-OCT) of idiopathic stage 2 eccentric macular hole (MH) (case 5). Initial M-OCT showed stage 2 eccentric MH (A). Two months after the first visit, M-OCT revealed closure of MH by retinal bridging with persis-tent subretinal fluid (B). Five months after the first visit, complete closure of MH was seen but defects at the photoreceptor in-ner/outer segment junction level remained (C). Complete PVD was observed during the process by slit-lamp funduscopic examination (not shown in the figure).
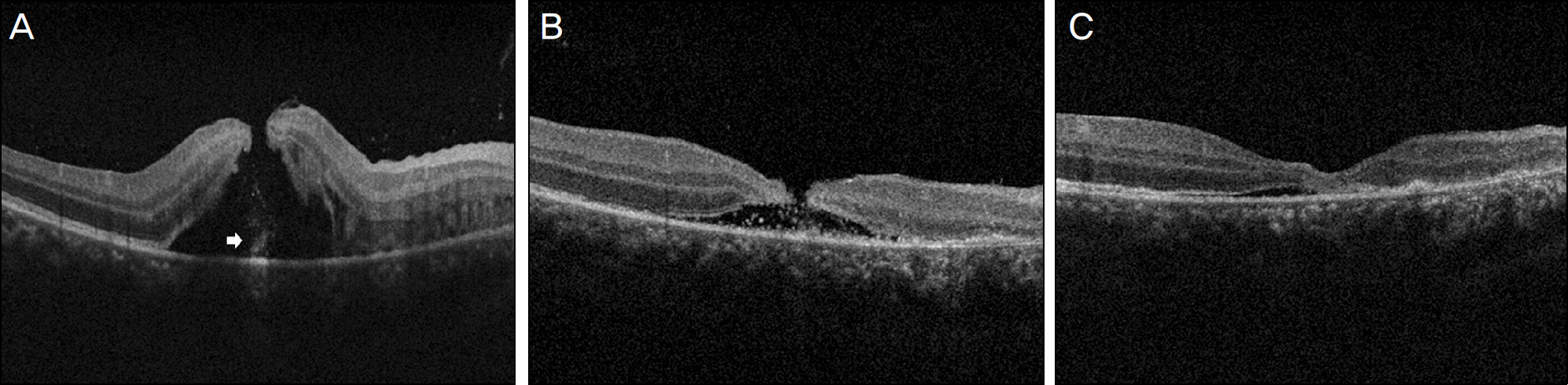
Figure 4. Optical coherence tomography (M-OCT) of traumatic macular hole (MH) (case 6). Initial M-OCT showed MH with sub-retinal hemorrhage (white arrow) and subretinal fluid (A). One week after the trauma, M-OCT revealed marked decreased MH size with decreased subretinal fluid (B). One month after the first visit, complete closure of MH was seen but small amounts of subretinal fluid persisted with irregular hyperreflectivity at the retinal pigment epithelium and photoreceptor inner/outer segment level (C).

Figure 5. Optical coherence tomography (M-OCT)of traumatic macular hole (MH) by electrical burn (case 8). The patient visited ophthalmologic department 3 months after the trauma with gradual progression of decreased visual acuity. M-OCT at the first visit showed MH and complete posterior vitreous detachment (white arrow) (A). One month after the first visit, M-OCT revealed de-creased MH size with decreased subretinal fluid (B). Five months after the first visit, complete closure of MH was seen but defect of photoreceptor inner/outer segment junction persisted (C).

Figure 6. Optical coherence tomography (M-OCT)of epiretinal membrane (ERM) with pseudohole (case 9). Initial M-OCT showed ERM with pseudohole and incomplete posterior vitreous detachment (PVD) (A). One month after the first visit, M-OCT revealed resolution of ERM with complete PVD, decreased size of pseudohole and intraretinal fluid (B). Nine months after the first visit, in-traretinal fluid further decreased but still persisted (C).
Reference
-
References
1. Barak Y, Ihnen MA, Schaal S. Spectral domain optical coherence tomography in the diagnosis and management of vitreoretinal in-terface pathologies. J Ophthalmol. 2012; 2012:876472.
Article2. Jaffe NS. Vitreous traction at the posterior pole of the fundus due to alternations in the vitreous posterior. Trans Am Acad Ophthalmol Otolaryngol. 1967; 71:642–52.3. Koizumi H, Spaide RF, Fisher YL. . Three-dimensional evalu-ation of vitreomacular traction and epiretinal membrane using spectral-domain optical coherence tomography. Am J Ophthalmol. 2008; 145:509–17.
Article4. Chang LK, Fine HF, Spaide RF. . Ultrastructural correlation of spectral-domain optical coherence tomography findings in vitre-omacular traction syndrome. Am J Ophthalmol. 2008; 146:121–7.5. Gandorfer A, Rohleder M, Kampik A. Epiretinal pathology of vit-reomacular traction syndrome. Br J Ophthalmol. 2002; 86:902–9.
Article6. Gallemore RP, Jumper JM, McCuen BW 2nd. . Diagnosis of vitreoretinal adhesions in macular disease with optical coherence tomography. Retina. 2000; 20:115–20.
Article7. Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular traction syndrome. Am J Ophthalmol. 1995; 119:55–61.
Article8. Odrobina D, Michaelswka Z, Michalewski J. . Long-term eval-uation of vitreomacular traction disorder in spectral-domain opti-cal coherence tomography. Retina. 2011; 31:324–31.
Article9. Michalewska Z, Cisiecki S, Sikorski B. . Spontaneous closure of stage III and IV idiopathic full-thickness macular holes-a two case report. Graefes Arch Clin Exp Ophthalmol. 2008; 246:99–104.10. Milani P, Seidenari P, Carmassi L, Bottoni F. Spontaneous reso-lution of a full thickness idiopathic macular hole: fundus auto-fluorescence and OCT imaging. Graefes Arch Clin Exp Ophthalmol. 2007; 245:1229–31.
Article11. Ishida M, Takeuchi S, Okisaka S. Optical coherence tomography images of idiopathic macular holes with spontaneous closure. Retina. 2004; 24:625–8.
Article12. García Fernández M, Castro Navarro J. Spontaneous closure of stage IV idiopathic full-thickness macular hole and late reopening as a lamellar macular hole: a case report. J Med Case Rep. 2012; 6:169.
Article13. Greven CM, Slusher MM, Weaver RG. Epiretinal membrane re-lease and posterior vitreous detachment. Ophthalmology. 1988; 95:902–5.
Article14. Reese AB, Jones IS, Cooper WC. Macular changes secondary to vitreous traction. Am J Ophthalmol. 1967; 64(Suppl):544–9.
Article15. Haouchine B, Massin P, Tadayoni R. . Diagnosis of macular pseudoholes and lamellar macular holes by optical coherence tomography. Am J Ophthalmol. 2004; 138:732–9.
Article16. Gass JD. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995; 119:752–9.
Article17. Yuzawa M, Watanabe A, Takahashi Y, Matsui M. Observation of idiopathic full-thickness macular holes: Follow-up observation. Arch Ophthalmol. 1994; 112:1051–6.18. Guyer DR, de Bustros S, Diener-West M, Fine SL. Observations on patients with idiopathic macular holes and cysts. Arch Ophthalmol. 1992; 110:1264–8.
Article19. Mizusawa Y, Ichibe M, Yoshizawa T, Ando N. Clinical evaluation of traumatic macular hole. Jpn Rev Clin Ophthalmol. 1996; 90:790–2.20. Tomii A, Ikeda N, Kurusu A, Mimura O. Clinical course of trau-matic macular hole. Jpn Rev Clin Ophthalmol. 1999; 53:1274–8.21. Yamashita T, Uemara A, Uchino E. . Spontaneous closure of traumatic macular hole. Am J Ophthalmol. 2002; 133:230–5.
Article22. Byer NE. Spontaneous disappearance of early postoperative pre-retinal traction. Arch Ophthalmol. 1973; 90:133–5.23. Meyer CH, Rodrigues EB, Mennel S. . Spontaneous separation of epiretinal membrane in young subjects: personal observations and review of the literature. Graefes Arch Clin Exp Ophthalmol. 2004; 242:977–85.
Article24. Guyer DR, de Bustros S, Diener-West M, Fine SL. Observations on patients with idiopathic macular holes and cysts. Arch Ophthalmol. 1992; 110:1264–8.
Article25. Freund KB, Ciardella AP, Shah V. . Optical coherence tomog-raphy documentation of spontaneous macular hole closure without posterior vitreous detachment. Retina. 2002; 22:506–9.
Article26. Lai MM, Bressler SB, Haller JA. Spontaneous resolution of mac-ular microhole. Am J Ophthalmol. 2006; 141:210–2.
Article27. Hwang DJ, Park KH, Woo SJ. Spontaneous resolution of vitre-omacular traction syndrome with persistent vitreofoveal adhesion observed on spectral-domain optical coherence tomography. Can J Ophthalmol. 2012; 47:e17–9.
Article28. Minihan M, Goggin M, Cleary PE. Surgical management of mac-ular holes: results using gas tamponade alone, or in combination with autologous platelet concentrate, or transforming growth fac-tor beta 2. Br J Ophthalmol. 1997; 81:1073–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vitreous Vascular Endothelial Growth Factor Concentration In Various Vitreoretinal Disorders
- Bilateral Spontaneous Resolution of Chronic Subdural Hematoma: A Case Report
- The Spontaneous Resolution of Idiopathic Macular Hole Diagnosed with OCT
- Mutational Profile of Vitreoretinal Lymphoma
- Rapid Spontaneous Resolution of Acute Subdural Hematoma
