A Case of Primary Orbital Synovial Sarcoma
- Affiliations
-
- 1Department of Ophthalmology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. eyeyang@inje.ac.kr
Abstract
- PURPOSE
To report a rare case of primary orbital synovial sarcoma.
CASE SUMMARY
A 55-year-old male visited our clinic with a 2-month history of decreased visual field in the left eye. The best corrected visual acuity of the left eye was 1.0, and 2.5 mm of proptosis was observed. There was slight limitations in motility and a mild visual field defect in the inferotemporal quadrant of the left eye. Funduscopic examination of the left eye revealed papilledema. Orbital magnetic resonance imaging (MRI) demonstrated the presence of an orbital mass that extended inferotemporally into the left orbit. On magnetic resonance imaging, a well-demarcated and 2.7 x 2.0 x 2.2 cm sized tumor was identified with intermediate signal intensities on T1/T2-weighted scans with slight homogenous enhancement. We approached the orbital mass using a lateral conjunctival incision with left canthotomy and cantholysis and performed partial surgical resection of the mass because the mass encircled the optic nerve. The mass was diagnosed as synovial sarcoma based on the findings of both histopathology and immunohistochemical staining. Postoperatively, the patient underwent radiation therapy to the rest of the tumor site.
CONCLUSIONS
Synovial sarcoma should be considered in the differential diagnosis of an orbital mass lesion encircling the optic nerve. Radiation therapy is useful to treat completely unresectable primary synovial sarcoma.
MeSH Terms
Figure
-
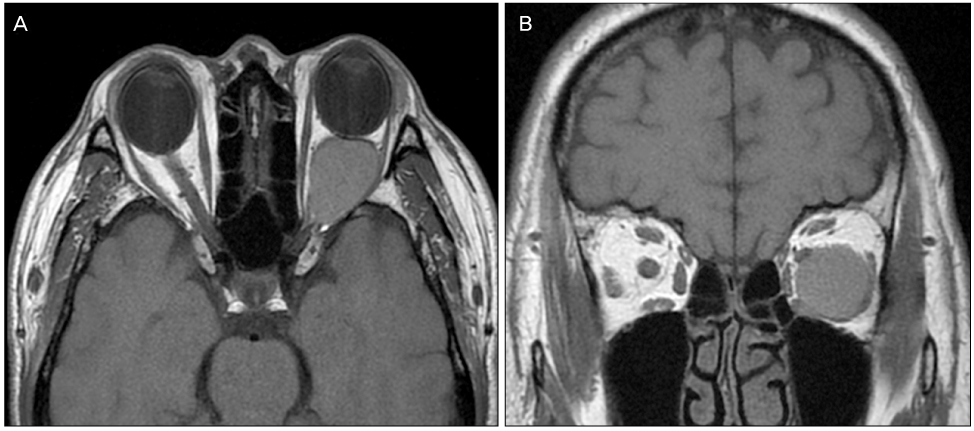
Figure 1 Magnetic Resonance Imaging of the left orbit demonstrates a large, homogenous, well-circumscribed mass in the retrobulbar space. The mass abuts onto the optic nerve and compresses it superomedially. Axial (A) and coronal (B) views.
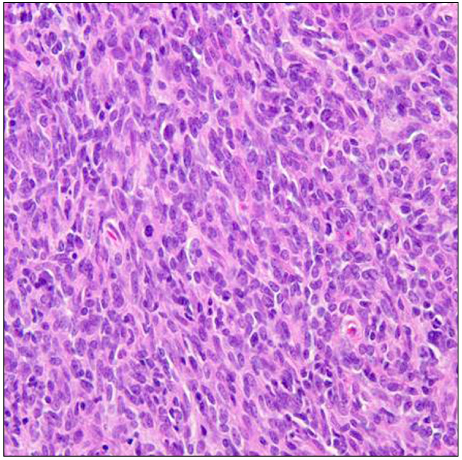
Figure 2 Higher magnification of the biphasic synovial sarcoma specimen (hematoxylin & eosin stain [H&E]; original magnification, ×400). The spindle cell component is elongated cells with spindled hyperchromatic nuclei and scant amounts of cytoplasm. The epithelioid cell component shows cuboidal to round cells with oval to round nuclei, abundant cytoplasm, and prominent nucleoli.

Figure 3 Higher magnification of the biphasic synovial sarcoma specimen (immunohistochemical stain; original magnification, ×200). (A) Vimentin immunohistochemical staining of the tissue shows diffuse and dense positivity in the spindle cell component. (B) Epithelial membrane antigen (EMA) immunohistochemical staining highlights the epithelial component of this biphasic synovial sarcoma.
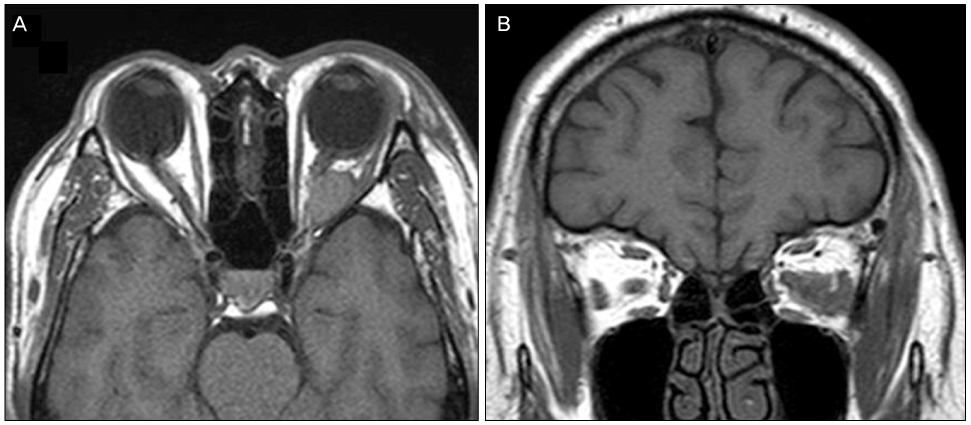
Figure 4 Magnetic Resonance Imaging of the left orbit shows known synovial sarcoma remnant. As compared with previous imaging, it was decreased more than 50% in volume (2.7 × 2.0 × 2.2 cm → 1.2 × 1.4 × 1.8 cm). Axial (A) and coronal (B) views.
Reference
-
1. Deshmukh R, Mankin HJ, Singer S. Synovial sarcoma: the importance of size and location for survival. Clin Orthop Relat Res. 2004. (419):155–161.2. Okcu MF, Munsell M, Treuner J, et al. Synovial sarcoma of childhood and adolescence: a multicenter, multivariate analysis of outcome. J Clin Oncol. 2003. 21:1602–1611.3. Rangheard AS, Vanel D, Viala J, et al. Synovial sarcomas of the head and neck: CT and MR imaging finding of eight patients. AJNR Am J Neuroradiol. 2001. 22:851–857.4. Schmidt D, Thum P, Harms D, Theuner J. Synovial sarcoma in children and adolescents. A report from the Kiel Pediatric Tumor Registry. Cancer. 1991. 67:1667–1672.5. Ratnatunga N, Goodlad JR, Sankarakumaran N, et al. Primary biphasic synovial sarcoma of the orbit. J Clin Pathol. 1992. 45:265–267.6. Buono LM, Silberschmidt A, Foroozan R, Savino PJ. Metastatic synovial sarcoma to the skull base and orbit. Am J Ophthalmol. 2002. 134:785–787.7. Shukla PN, Pathy S, Sen S, et al. Primary orbital calcified synovial sarcoma: a case report. Orbit. 2003. 22:299–303.8. Hartstein ME, Silver FL, Ludwig OJ, O'Connor DM. Primary synovial sarcoma. Ophthalmology. 2006. 113:2093–2096.9. Kusuma S, Skarupa DJ, Ely KA, et al. Synovial sarcoma of the head and neck: a review of its diagnosis and management and a report of a rare case of orbital involvement. Ear Nose Throat J. 2010. 89:280–283.10. Lee SH, Chang MH, Baek KK, et al. High-dose Ifosfamide as second- or third-line chemotherapy in refractory bone and soft tissue sarcoma patients. Oncology. 2011. 80:257–261.11. Helman LJ, Meltzer P. Mechanisms of sarcoma development. Nat Rev Cancer. 2003. 3:685–694.
