Comparison of Outcomes of Femtosecond Laser-assisted Keratoplasty and Conventional Penetrating Keratoplasty
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, Seoul St. Mary's Hospital, The Catholic University of Korea School of Medicine, Seoul, Korea. ckjoo@catholic.ac.kr
- 2Department of Ophthalmology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3The Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
Abstract
- PURPOSE
To compare the outcomes of IntraLase femtosecond laser-enabled keratoplasty (IEK) versus conventional penetrating keratoplasty (C-PKP).
METHODS
This retrospective study included 18 eyes of 17 patients who underwent C-PKP and 26 eyes of 25 patients who underwent IEK. Postoperative clinical results were compared between two groups.
RESULTS
The mean logMAR best spectacle-corrected visual acuity (BSCVA) was 0.70, 0.58, and 0.61 in the IEK group, and 1.06, 1.01, and 0.90 in the C-PKP group at postoperative 2, 4, and 6 months respectively. The difference between the two groups was statistically significant at 2 and 4 months postoperatively (p=0.033, 0.011). The mean refractive cylinder was 4.08 diopters (D), 4.01D, and 4.44D in the IEK group, while 5.75D, 5.75D, and 5.21D in the C-PKP group for each month, and the difference between the groups was statistically significant at 2 and 4 months postoperatively (p=0.037, 0.027). The complication rate showed no significant differences up to 6 months of follow-up between the two groups.
CONCLUSIONS
The IEK showed better results in BSCVA and refractive astigmatism in the early postoperative period, in comparison with the C-PKP, and can be considered as a valuable method in penetrating keratoplasty.
MeSH Terms
Figure
-

Figure 1. Illustration of the 4 wound configurations created in this study by the IntraLase-enabled keratoplasty (IEK) software: traditional, straight vertical cut (A), Top hat (B), musch-room (C), Z-square (D).
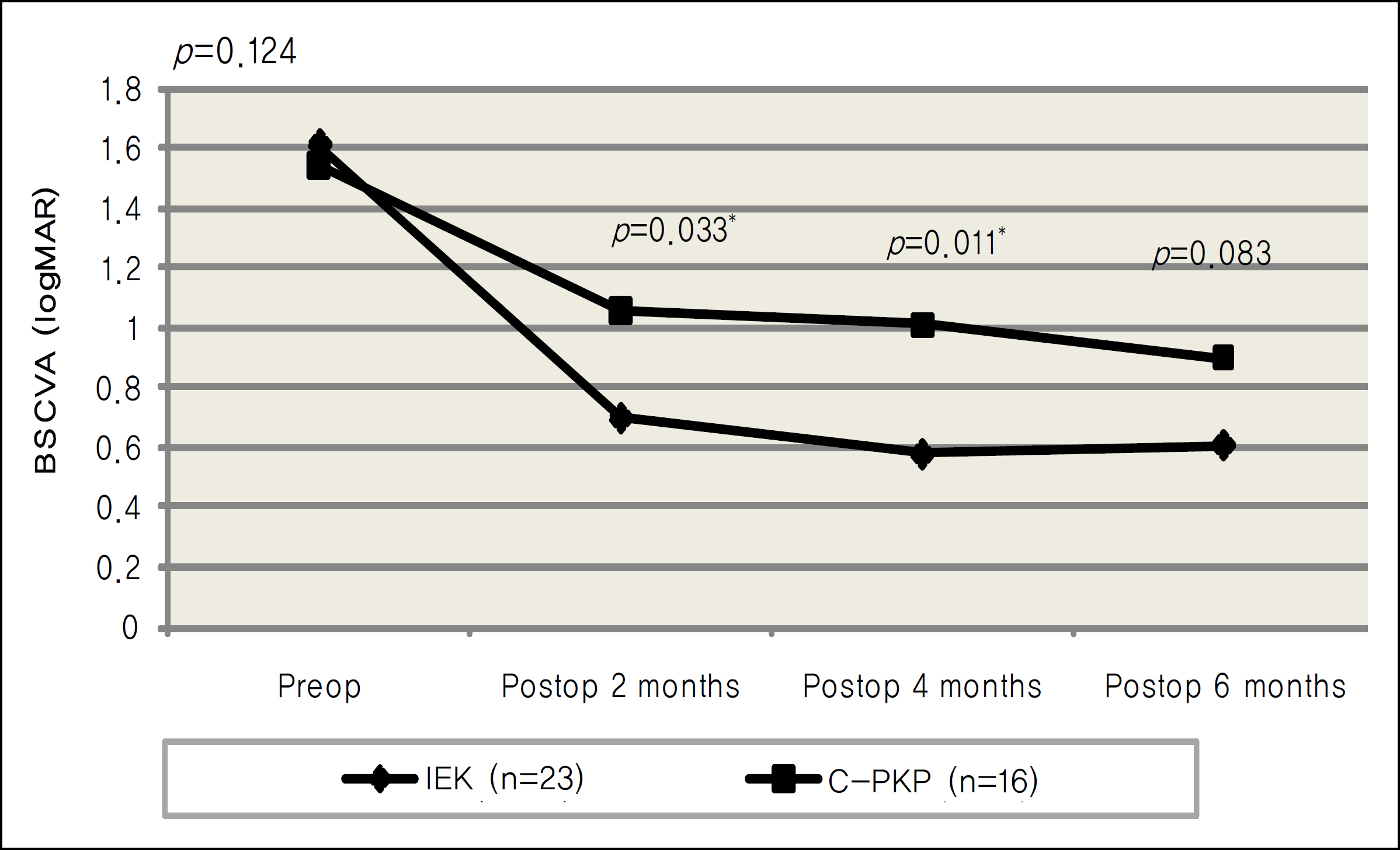
Figure 2. Postoperative changes of logMAR mean best-spectacle corrected visual acuity (BSCVA) after IntraLase-enabled keratoplasty (IEK) versus conventional penetrating keratoplasty (C-PKP); Postoperative BSCVA improved gradually in both groups. BSCVA in IEK group was better than C-PKP group postoperatively, but the differences between two groups were statistically significant at 2 months (p=0.033), and 4 months (p=0.011) postoperatively. The statistical analysis was performed using Mann-Whitney U test. A P-value less than 0.05 is statistically significant.

Figure 3. The cylinder measured using autorefractor in both groups of IntraLase-enabled keratoplasty (IEK) and conventional penetrating keratoplasty (C-PKP) at 2, 4 and 6 months postoperatively. The refractive cylinder showed lower value in IEK during follow up periods, and the difference was statistically significant at 2 months (p=0.037), and 4 months (p=0.027) postoperatively (A). The keratometric cylinder measured using manual keratometer showed lower value in IEK than C-PKP, but the difference was not statistically significant during follow up periods (B). The statistical analysis was performed using Mann-Whitney U test. A P-value less than 0.05 is statistically significant.
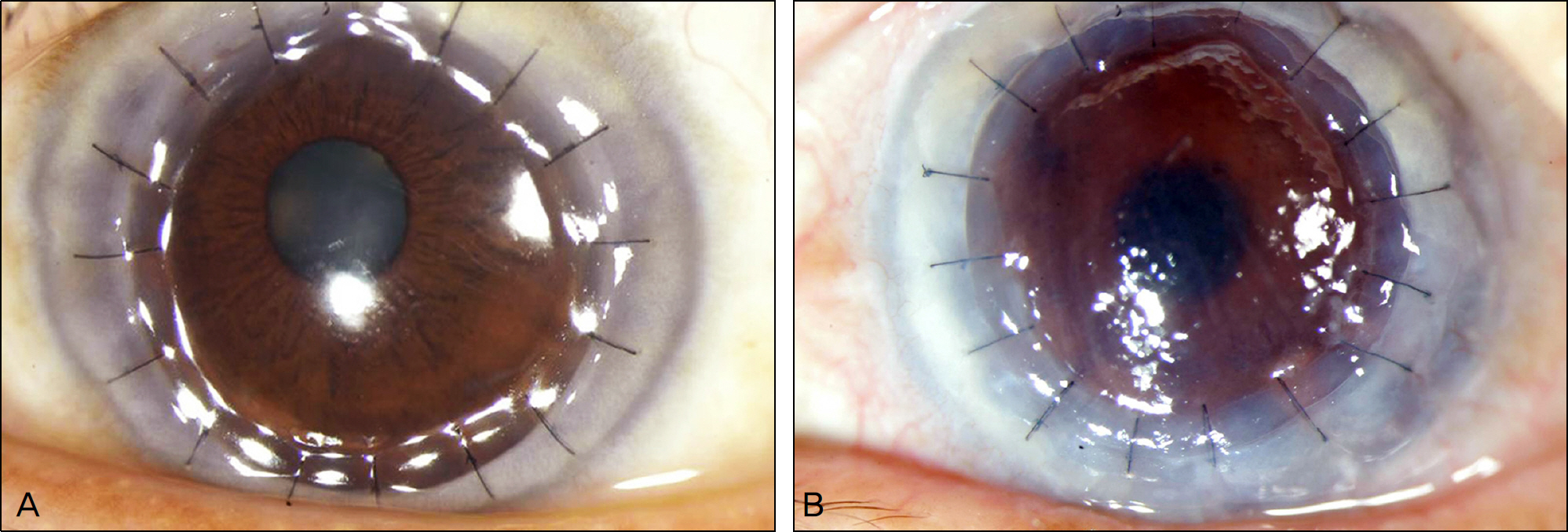
Figure 4. Anterior segment photographs of the patients at 1 month after surgery show the clear central cornea with well attached peripheral flange in Intralase-enabled keratoplasty (vertical cut) (A), and moderately edematous cornea with well attached graft in conventional penetrating keratoplasty (B).
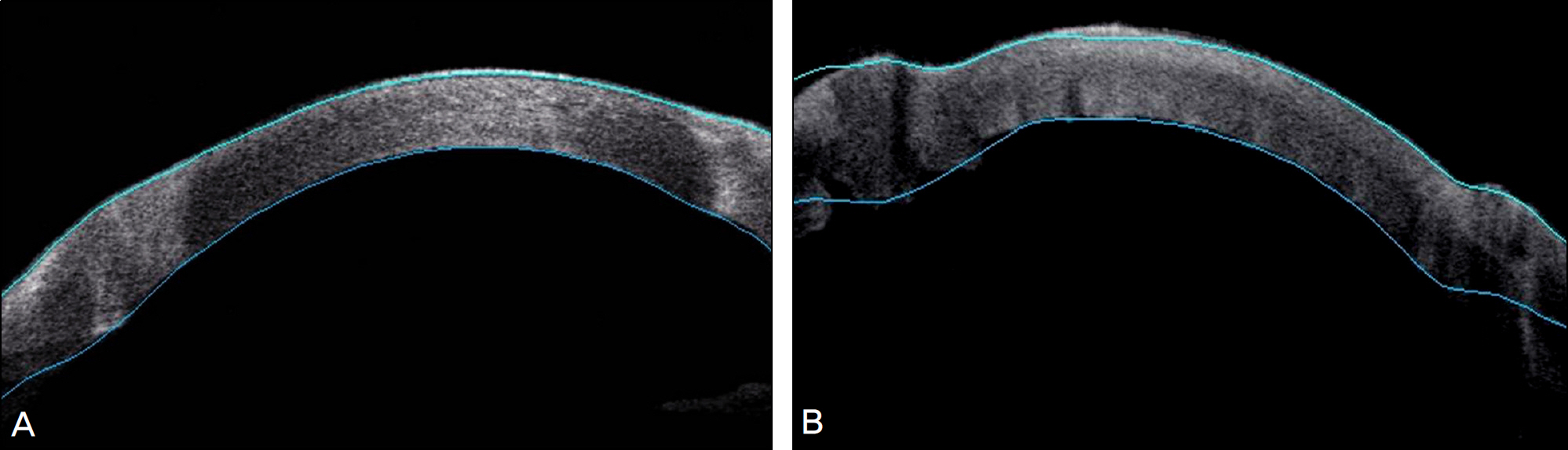
Figure 5. Two months postoperatively, Visante optical coherence tomography of Intralase-enabled keratoplasty (vertical type) (A), demonstrating the perfect match of the recipient to the donor. In contrast, conventional penetrating keratoplasty (B) may show the lack of precise match of cut between the two pieces of tissues and protrusions such as hills.
Reference
-
References
1. Ing JJ, Ing HH, Nelson LR, et al. Ten-year postoperative results of penetrating keratoplasty. Ophthalmology. 1998; 105:1855–65.
Article2. Thompson RW Jr, Price MO, Bowers PJ, Price FW Jr. Long-term graft survival after penetrating keratoplasty. Ophthalmology. 2003; 110:1396–402.
Article3. Kaiserman I, Bahar I, Rootman DS. Corneal wound malapposition after penetrating keratoplasty: an optical coherence tomography study. Br J Ophthalmol. 2008; 92:1103–7.
Article4. Farid M, Kim M, Steinert RF. Results of penetrating keratoplasty performed with a femtosecond Laser zigzag incision initial report. Ophthalmology. 2007; 114:2208–12.
Article5. Ignacio TS, Nguyen TB, Chuck RS, et al. Top hat wound configuration for penetrating keratoplasty using the femtosecond laser: a laboratory model. Cornea. 2006; 25:336–40.6. Frost NA, Wu J, Lai TF, Coster DJ. A review of randomized controlled trials of penetrating keratoplasty techniques. Ophthalmology. 2006; 113:942–9.
Article7. Barraquer JI Jr. Technique of penetrating keratoplasty. Am J Ophthalmol. 1950; 33:6–17.
Article8. Binder PS, Abel R Jr, Polack FM, Kaufman HE. Keratoplasty wound separations. Am J Ophthalmol. 1975; 80:109–15.
Article9. Farley MK, Pettit TH. Traumatic wound dehiscence after penetrating keratoplasty. Am J Ophthalmol. 1987; 104:44–9.
Article10. Rehany U, Rumelt S. Ocular trauma following penetrating keratoplasty: incidence, outcome, and postoperative recommendations. Arch Ophthalmol. 1998; 116:1282–6.11. Tseng SH, Lin SC, Chen FK. Traumatic wound dehiscence after penetrating keratoplasty: clinical features and outcome in 21 cases. Cornea. 1999; 18:553–8.12. Melles GR, Lander F, van Dooren BT, et al. Preliminary clinical results of posterior lamellar keratoplasty through a sclerocorneal pocket incision. Ophthalmology. 2000; 107:1850–6.13. Alio JL, Shah S, Barraquer C, et al. New techniques in lamellar keratoplasty. Curr Opin Ophthalmol. 2002; 13:224–9.
Article14. Mearza AA, Qureshi MA, Rostron CK. Experience and 12-month results of Descemet-stripping endothelial keratoplasty (DSEK) with a small-incision technique. Cornea. 2007; 26:279–83.
Article15. Busin M. A new lamellar wound configuration for penetrating keratoplasty surgery. Arch Ophthalmol. 2003; 121:260–5.
Article16. Malta JB, Soong HK, Shtein R, et al. Femtosecond Laser-assisted keratoplasty: laboratory studies in eye bank eyes. Curr Eyes Res. 2009; 34:18–25.
Article17. Stern D, Schoenlein RW, Puliafito CA, et al. Corneal ablation by nanosecond, picosecond, and femtosecond lasers at 532 and 625 nm. Arch Ophthalmol. 1989; 107:587–92.
Article18. Bahar I, Kaiserman I, McAllum P, Rootman D. Femtosecond laser-assisted penetrating keratoplasty stability evaluation of different wound configurations. Cornea. 2008; 27:209–11.19. Price FW, Price MO. Adult keratoplasty: has the prognosis improved in the last 25 years? Int Ophthalmol. 2008; 28:141–6.20. Bahar I, Kaiserman I, Lange AP, et al. Femtosecond laser versus manual dissection for top hat penetrating keratoplasty. Br J Oophthalmol. 2009; 93:73–8.
Article21. Claesson M, Armitage WJ. Astigmatism and the impact of relaxing incisions after penetrating keratoplasty. J Refract Surg. 2007; 23:284–9.
Article22. Sohn BJ, Kim HK. Early results of Femtosecond laser-assisted mushroom-shaped wound-configurized keratoplasty. J Korean Ophthalmol Soc. 2009; 50:34–43.
Article23. Price FW Jr., Price MO, Jordan CS. Safety of incomplete incision patterns in femtosecond laser-assisted penetrating keratoplasty. J Cataract Refract Surg. 2008; 34:2099–103.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the Long-term Clinical Outcomes of Penetrating Keratoplasty Using a Manual Trephine and Femtosecond-Laser Trephination
- A Case Report of Fungal Keratitis Diagnosed by Femtosecond Laser Assisted Corneal Biopsy
- Early Results of Femtosecond Laser-Assisted Mushroom-Shaped Wound-Configurized Keratoplasty
- Early Result of Femtosecond Laser Assisted Descemet's Membrane Stripping Endothelial Keratoplasty
- Cataract Extraction after Penetrating Keratoplasty
