Clinical Features of Ocular Disabilities
- Affiliations
-
- 1Department of Ophthalmology, The Dankook University Medical College, Cheonan, Korea. kseeye@hanmail.net
Abstract
- PURPOSE
To describe the characteristics of the disabled patients visiting the eye clinic in our institute.
METHODS
We carried out a retrospective analysis of 35 cases in our clinic from April 2004 to June 2008 using the McBride disability evaluation. We investigated the clinical features and the causes of disorders through visual acuity, visual field and ocular motility.
RESULTS
Thirty-three (94.3%) of the 35 patients had disabilities due to trauma; twelve (34.3%) of them were caused by traffic accidents, and 21 (60%) of them were due to blows or lacerations. Other causes of disability were glaucoma and retinal break (5.8%). Nine patients (25.7%) had abnormal findings in the visual field examination, and nine other patients (25.7%) had limitations in ocular motility. Twenty-eight patients (80%) had decreased visual acuity, and nine (25.7%) had multiple symptoms.
CONCLUSIONS
Considering the contribution of disability estimation of visual field and ocular motility in McBride disability evaluations, we considered the importance of repetitive examinations and evaluations. When patients complained of unexplained decreased visual acuity with no anatomical abnormalities, multifocal ERG and multifocal VEP should be considered in order to distinguish it from malingering or functional visual loss.
Keyword
MeSH Terms
Figure
-
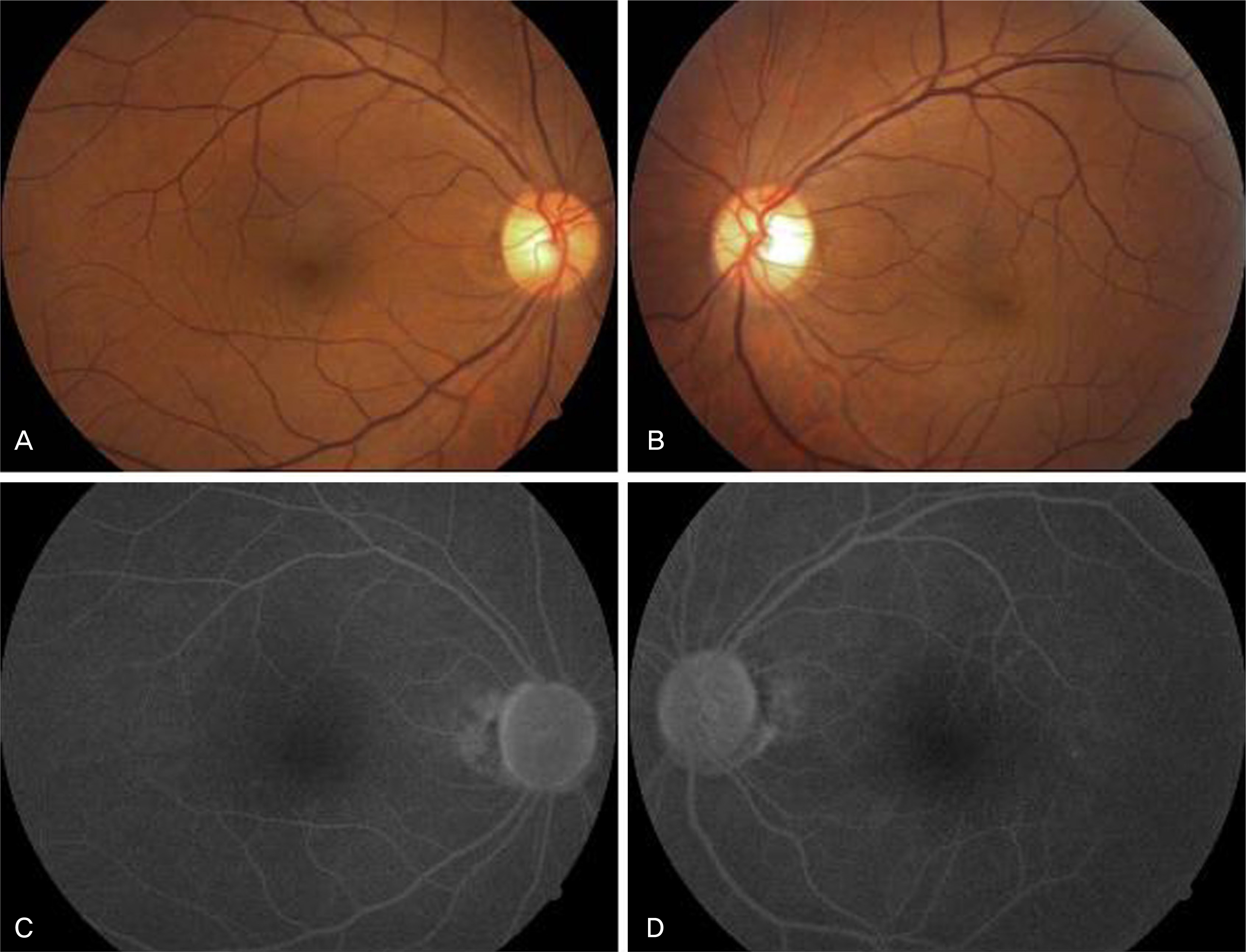
Figure 1. Fundus findings of case 1. The color fundus photos (A, B) and fluorescein angiographs (C, D) show nonspecific findings.

Figure 2. The visual evoked potential findings of case 1. The pattern visual evoked potential of the patient's left eye shows slightly delayed latency compared to that of his right eye.

Figure 3. The optical coherent tomography findings of case 1. The patient's retinal nerve fiber layer analysis shows normal findings.
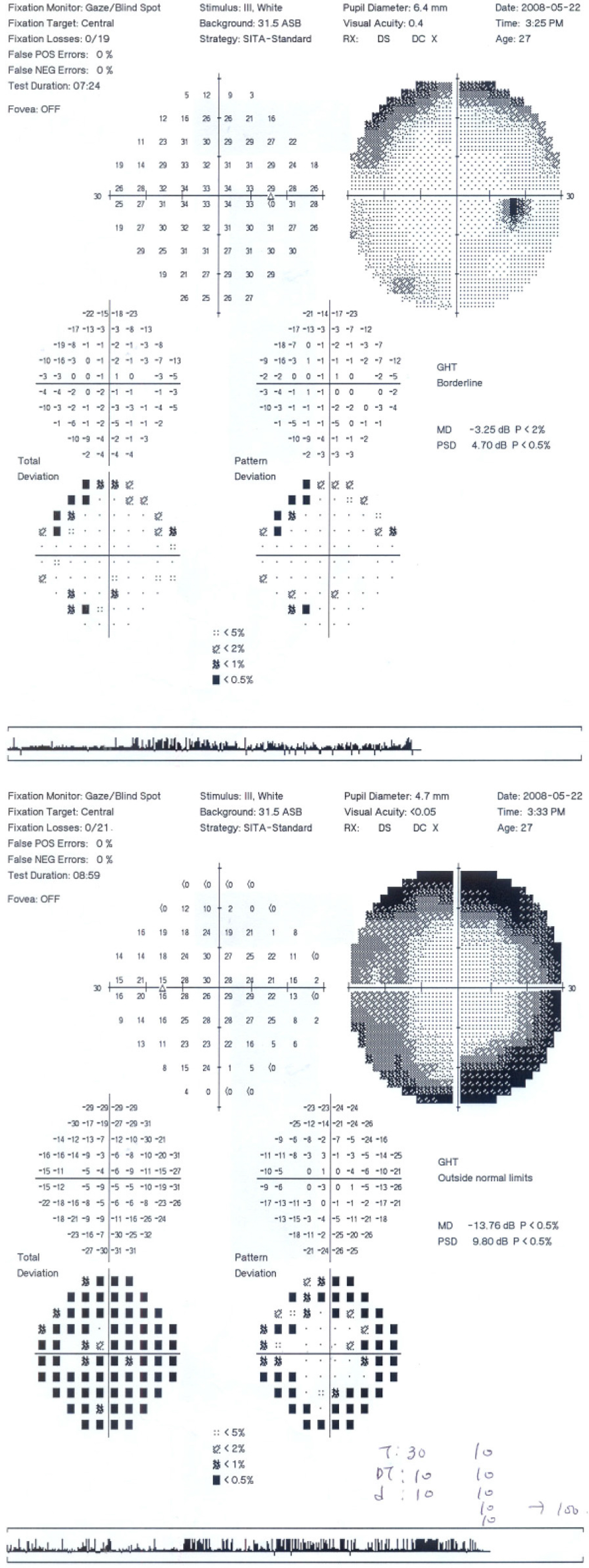
Figure 4. The visual field findings of case 2. The visual field shows peripheral constriction and suggestive malingering.
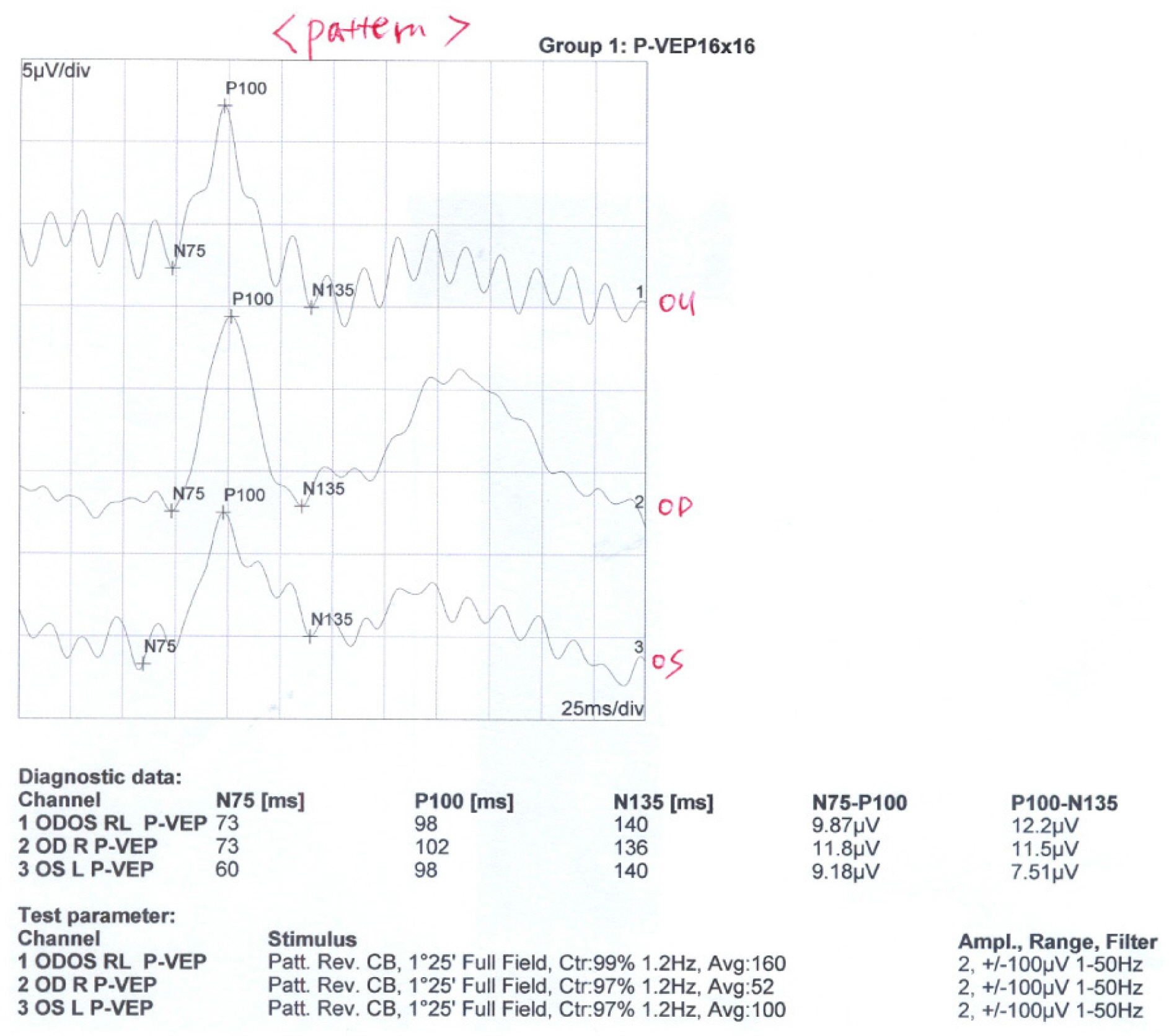
Figure 5. The visual evoked potential findings of case 2. The pattern visual evoked potential of the left eye shows slightly decreased amplitude compared to that of his right eye.

Figure 6. The optical coherent tomography findings of case 2. The patient's retinal nerve fiber layers analysis shows normal findings.
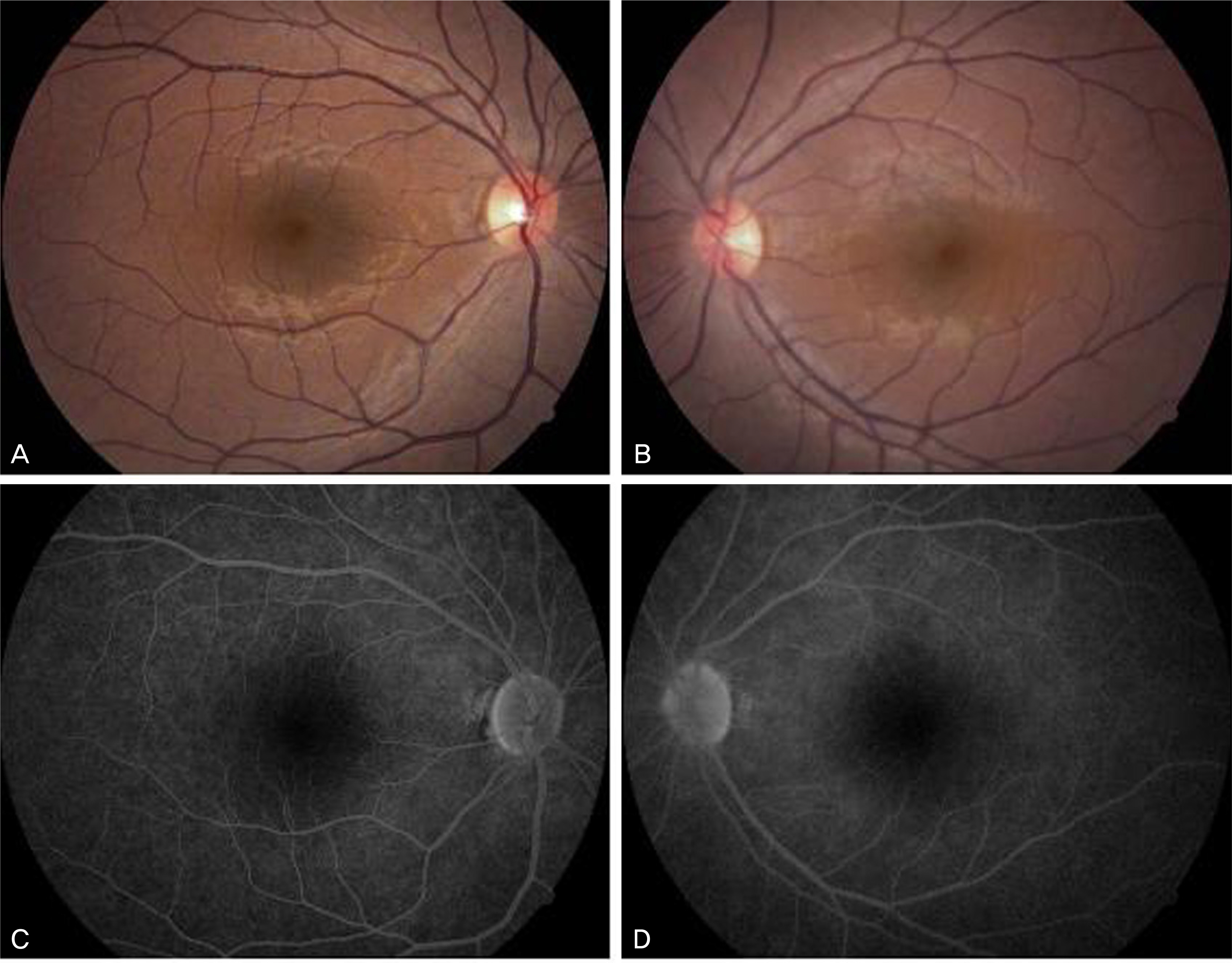
Figure 7. The fundus findings of case 2. The color fundus photos (A, B) and fluorescein angiography (C, D) show nonspecific findings.
Reference
-
References
1. Kim SY, Lee DH, Park SH. An analysis of visual fields in patients with posttraumatic functional visual loss. J Korean Ophthalmol Soc. 2004; 45:469–79.2. Kim CH. A Study on the Reform of the Physical Disability aberrations System of Korea. Seoul: Kunkuk University Graduate School;2005. p. 9–11.3. Massof RW. The measurement of vision disability. Optom Vis Sci. 2002; 79:516–52.
Article4. McBride DE. Disability Evaluation and Principles of Treatment of compensable Injuries: Injury of The eye. 6th ed.Philadelphia: Lippincott;1968. p. 465–79.5. Ohn YH, Ahn YS. Clinical applications of multifocal aberrations (mfERG). J Korean Ophthalmol. 2002; 43:1901–17.6. Park YT, Park SH, Shin HH. Problems of application to McBride disability evaluation in loss of visual efficiency patients. J Korean Ophthalmol. 1997; 38:1273–9.7. Park MJ, Lim SH, Lee SJ, Park SH. The effectiveness of visual evoked potentials in disability evaluation. J Korean Ophthalmol. 2006; 47:283–91.8. Xu S, Meyer D, Yoser S, et al. Pattern visual evoked potential in the diagnosis of functional visual loss. Ophthalmology. 2001; 108:76–81.9. False M, Mohn G. Assessment of visual function in suspected aberrations malingering. Br J Ophthalmol. 1989; 73:651–4.10. Gruber H. Decrease of visual acuity in patients with clear media and normal fundi. Objective screening methods for differentiation and documentation. Doc Ophthalmol. 1984; 56:327–35.
Article11. Hood DC. Assessing Retinal Function with the Multifocal aberrations. Prog Retin Eye Res. 2000; 19:607–46.12. Baek SC, Kim DK, Kang SM, Ohn YH. Multifocal electroretinograms in amblyopic patients. J Korean Ophthalmol Soc. 2005; 46:1313–20.13. Sutter EE, Tran D. The field topography of ERG components in man-I. The Photopic luminance response. Vision Res. 1992; 32:433–6.
Article14. Kim DK, Park TK, Ohn YH. Changes of multifocal electroretinograms after macular hole surgery. J Korean Ophthalmol Soc. 2005; 46:1351–60.15. Hood DC, Seiple W, Holopigian K, Greenstein V. A Comparison of the components of the multifocal and full-field ERGs. Vis Neurosci. 1997; 14:533–44.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- How Must We Prepare in the Next Decades When Caring for Those With Developmental Disabilities: “Grown Up” (2018)
- Why Fast COVID-19 Vaccination Needed for People with Disabilities and Autistics in Korea?
- Causes and Trends of Disabilities in Community-Dwelling Stroke Survivors: A Population-Based Study
- Clinical Features and Preventions of Ocular Injuries Associated With Mistaken Use of Superglue as Eyedrops
- Diabetes in People with Disabilities: a Call for Action
