An Incidental Finding of Pseudoexfoliation in Patient With Ophthalmic Artery Occlusion
- Affiliations
-
- 1Department of Ophthalmology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. ophdrkim@schch.ac.kr
Abstract
- PURPOSE
To report a case of pseudoexfoliation in the unaffected eye in a patient with ophthalmic artery occlusion.
CASE SUMMARY
A 49-year-old female presented with sudden vision loss in her right eye. On the initial examination, best corrected visual acuity was 20/500 in the right eye, and 20/20 in the left eye. Intraocular pressure in both eyes was 17 mmHg. Fundus examination showed retinal edema and a cotton wool spot in the right eye. There was a filling delay of choroidal and retinal vessels in the fluorescein angiography. On the slit lamp examination, there was pseudoexfoliation material around the pupil margin and lens capsule in the unaffected eye but no evidence of glaucoma. At the six-month follow-up, best corrected visual acuity in the right eye improved to 20/30 and a retinal nerve fiber layer defect was found at the spot of the previous cotton wool spot. On the visual field examination, visual defects corresponded with a retinal nerve fiber layer defect.
CONCLUSIONS
Pseudoexfoliation may be related to a systemic vascular disorder.
MeSH Terms
Figure
-
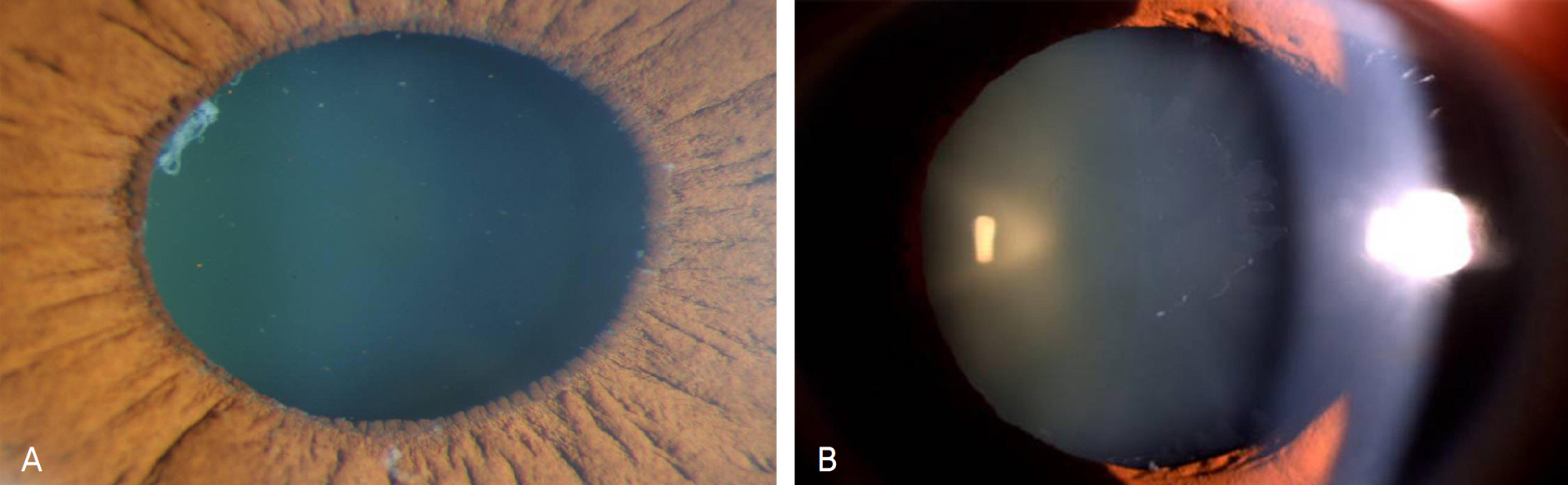
Figure 1. Anterior segment photographs of the left eye. (A) and (B): Pseudoexfoliative material deposition with curled edge on the anterior lens capsule.
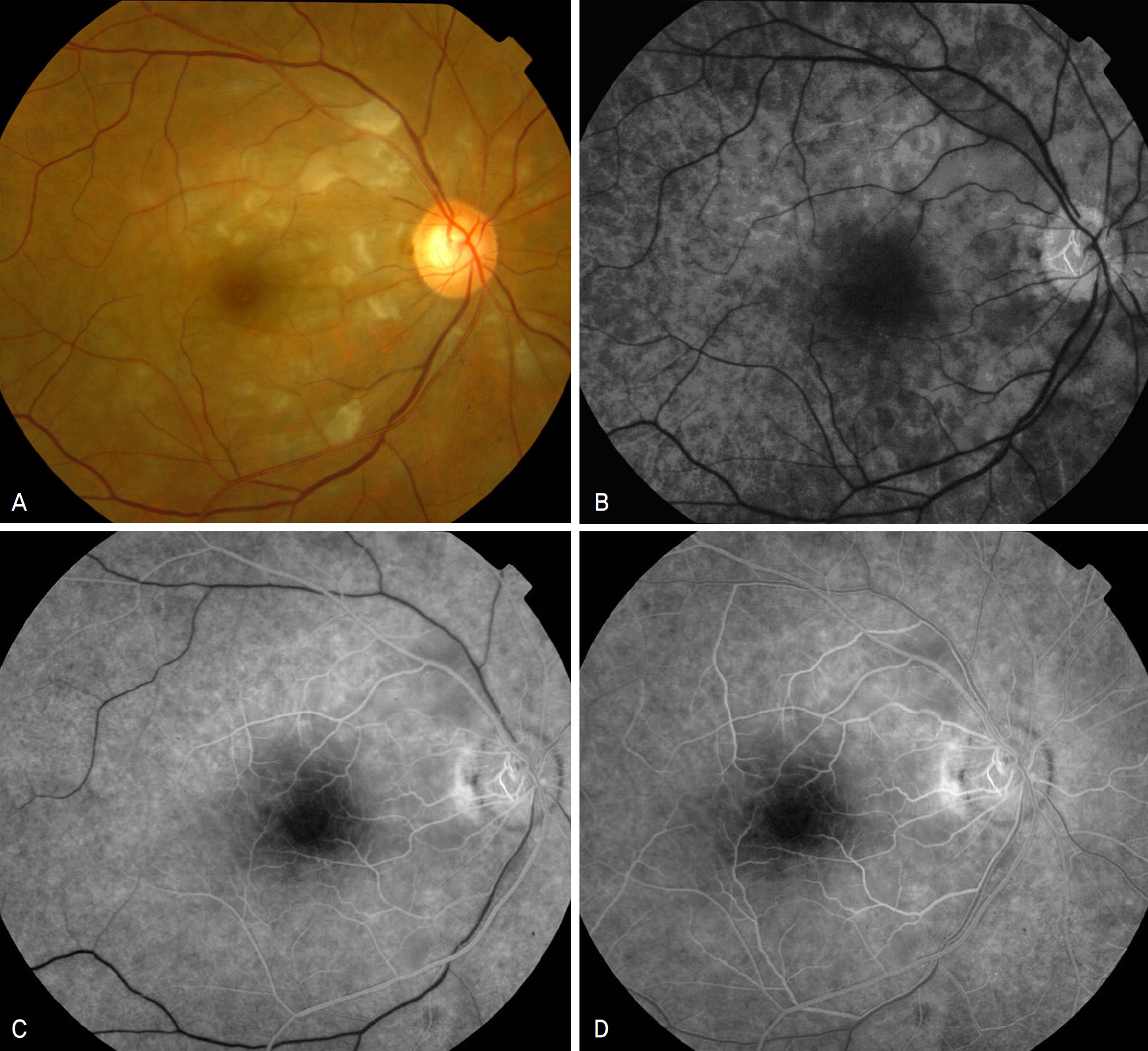
Figure 2. The Fundus photograph (A) and fluorescein angiographs of the right eye at the initial visit (B: 19.7 sec; C: 41.4 sec; D: 52.1 sec). Marked filling delay in nearly whole retinal and choroidal circulation.
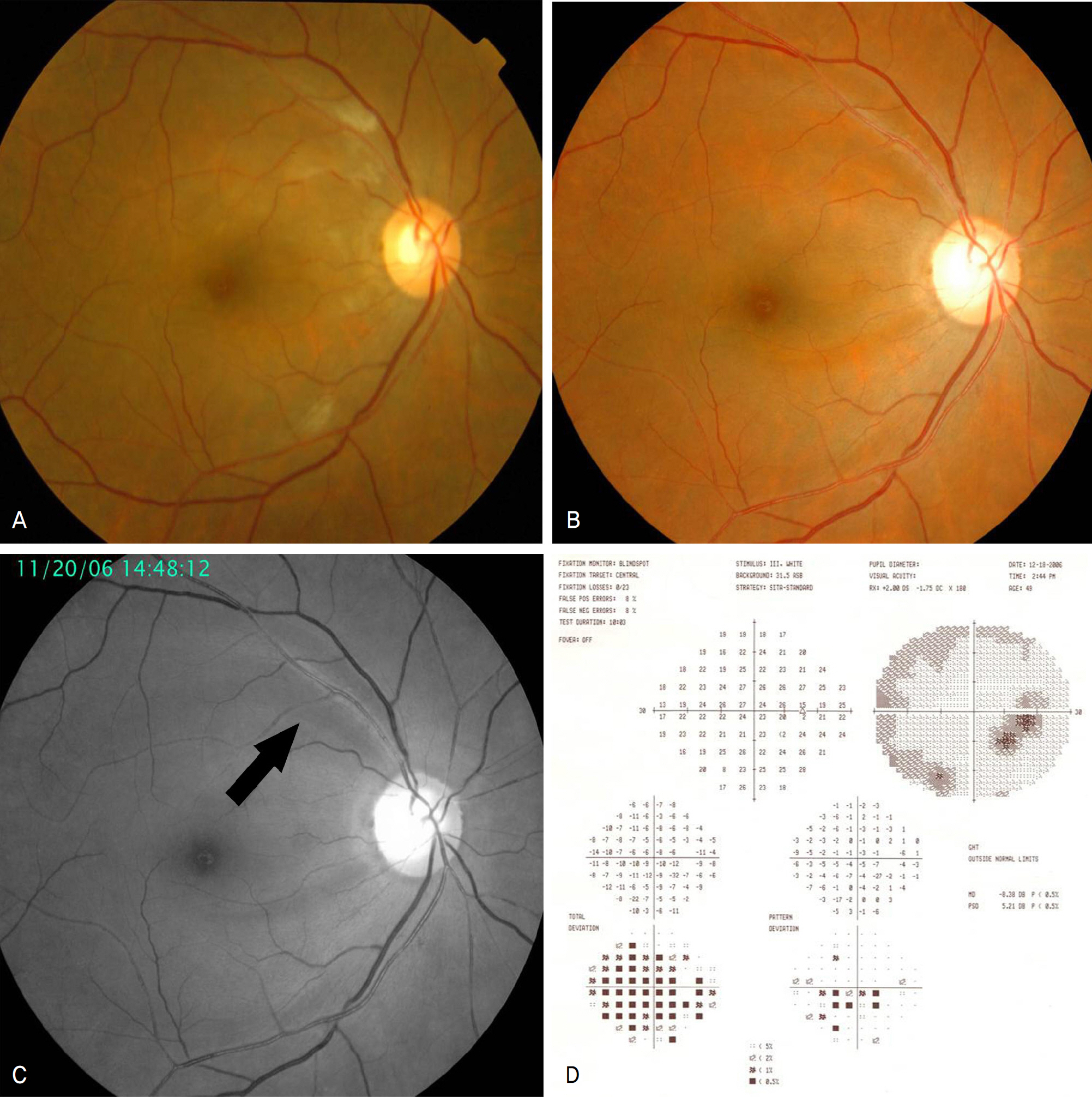
Figure 3. (A) and (B): Fundus photographs of the affected eye after 2 months and 6 months, respectively. The photographs show decreased cotton wool spots and retinal edema. (C) Red-free photograph after 6 months shows a retinal nerve fiber layer defect on the superior temporal area. (D) Humphrey perimetry after 6 months shows an arcuate visual field defect on the inferior temporal area.
Reference
-
References
1. Schlötzer-Schrehardt U, Naumann GO. Ocular and Systemic Pseudoexfoliation Syndrome. Am J Ophthalmol. 2006; 141:921–37.
Article2. Choi J, Park KH. Clinical characteristics of Korean patients with Pseudoexfoliation syndrome. J Korean Ophthalmol Soc. 2006; 47:577–86.3. Brooks AM, Gillies WE. The presentation and prognosis of glaucoma in pseudoexfoliation of the lens capsule. Ophthalmology. 1988; 95:271–6.
Article4. Naumann GO, Schlötzer-Schrehardt U, Küchle M. Pseudoexfoliation syndrome for the comprehensive ophthalmologist: Intraocular and systemic manifestations. Ophthalmology. 1998; 105:951–68.5. Ritch R, Schlötzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. 2001; 45:265–315.
Article6. Streeten BW, Li ZY, Wallace RN, et al. Pseudoexfoliative fibrillo-pathy in visceral organs of a patient with pseudoexfoliation syndrome. Arch Ophthalmol. 1992; 110:1757–62.
Article7. Schlötzer-Schrehardt UM, Koca MR, Naumann GO, Volkholz H. Pseudexfoliation syndrome. Ocular manifestation of a systemic disorder? Arch Ophthalmol. 1992; 110:1752–6.8. Lee MJ, Park YG, Ahn JK. Isolated cilioretinal artery occlusion in pseudoexfoliation syndrome: a case report. J Korean Ophthalmol Soc. 2006; 47:1686–90.9. Yazdani S, Tousi A, Pakravan M, Faghihi AR. Sensorineural hearing loss in pseudoexfoliation syndrome. Ophthalmology. 2008; 115:425–9.
Article10. Mitchell P, Wang JJ, Smith W. Association of pseudoexfoliation syndrome with increased vascular risk. Am J Ophthalmol. 1997; 124:685–67.
Article11. Lima VC, Prata TS, Liebmann JM, Ritch R. Central retinal artery occlusion and non-arteritic anterior ischemic optic neuropathy associated with an overlap syndrome: a case report. J Med Case Reports. 2008; 2:389.
Article12. Puska PM. Unilateral exfoliation syndrome: Conversion to bilateral exfoliation and to glaucoma-a prospective 10-year follow up study. J Galucoma. 2002; 11:517–24.13. Kivelä T, Hietanen J, Uusitalo M. Autopsy analysis of clinically unilateral exfoliation syndrome. Invest Ophthalmol Vis Sci 38. 1997; 38:2008–15.14. Hammer T, Schlötzer-Schrehardt U, Naumann GO. Unilateral or asymmetric pseudoexfoliation syndrome? An ultrastructural study. Arch Ophthalmol. 2001; 119:1023–31.15. Ritland JS, Egge K, Lydersen S, et al. Exfoliative glaucoma and primary open-angle glaucoma: associations with death causes and comorbidity. Acta Ophthalmol Scand. 2004; 82:401–4.
Article16. Bleich S, Jünemann A, von Ahsen N, et al. Homocysteine and risk of open-angle glaucoma. J Neural Transm. 2002; 109:1499–504.
Article17. Vessani RM, Ritch R, Liebmann J, Jofe M. Plasma homocystein is elevated in patients with exfoliation syndrome. Am J Ophthalmol. 2003; 136:41–6.18. Roedl JB, Bleich S, Reulbach U, et al. Vitamine deficiency and hyper-homocysteinemia in pseudoexfoliation glaucoma. J Neural Transm. 2007; 114:571–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ophthalmic Artery Occlusion After Carotid Revascularization
- Isolated Cilioretinal Artery Occlusion in Pseudoexfoliation Syndrome: A Case Report
- Association with Systemic and Ophthalmic Disease in Korean Pseudoexfoliation Syndrome Patients
- Incomplete Central Retinal Artery Occlusion
- Successful Endovascular Thrombectomy in a Patient with Monocular Blindness Due to Thrombus of the Ophthalmic Artery Orifice
