Rapid Spontaneous Regression of Bilateral Pseudotumor
- Affiliations
-
- 1Department of Ophthalmology, Gangwon National University, College of Medicine, Gangwon, Korea. opticus@kangwon.ac.kr
Abstract
- PURPOSE: To report a rare case of bilateral pseudotumor with a two-week rapid spontaneous regression Method: A 63-year-old man visited our clinic with a chief complaint of a headache and right ocular pain. An orbital computerized tomography (CT) scan revealed a roud mass with well-demarcated capsule-like boundaries located in the inferior part of both orbits. After a systemic evaluation to exclude a systemic malignancy, we performed excisional biopsy of the right orbital mass to make diagnosis. Result: The right orbital mass was not found at the time of surgery for an excisional biopsy. Instead, we took multiple small biopsies of orbital fat, inferior rectus muscle, and adjacent soft tissues. Histologic examination revealed a non-specific inflammatory reaction without the presence of tumor cells. There was a marked spontaneous regression of the mass in both orbits on an immediate follow-up orbital CT. The patient began steroid treatment for 12 weeks under the presumptive diagnosis of bilateral pseudotumor. There was no evidence of recurrence at the eight-month follow-up.
Figure
-

Figure 1. Pre-operative CT and MRI findings (2 weeks before excision al biopsy). Post-enhancement axial (A) and coronal (B) CT scan show the right eyeball is protruded compared with the left eyeball and homogenous, subtle enhanced, well demarcated round orbital mass in the inferior aspect of the globe. The both orbital mass is extending from the apex to the posterior margin of the globe (white arrows). There are displaced inferior rectus muscles not separable from the mass and no adjacent bone destruction.
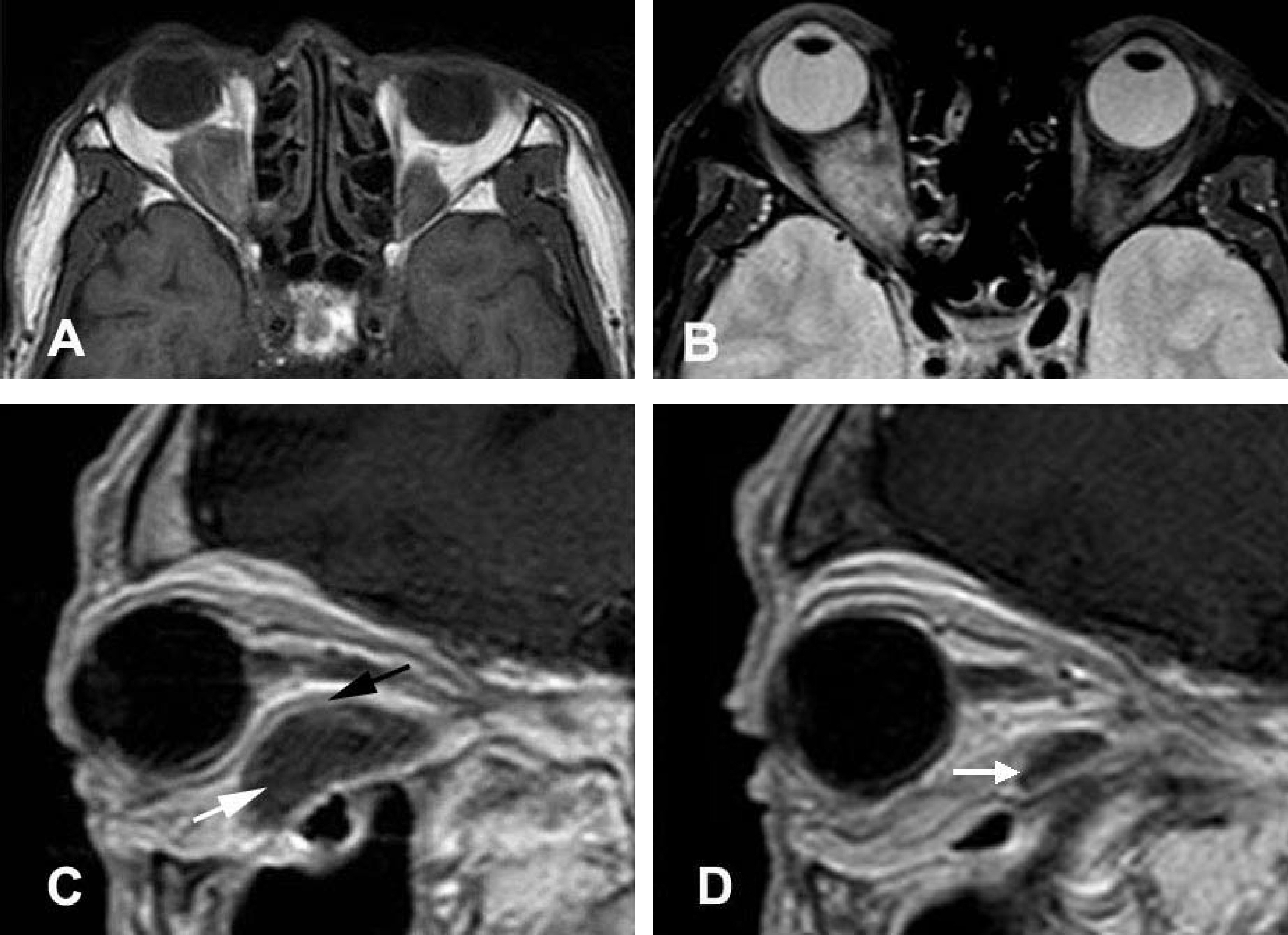
Figure 2. Pre-operative MRI findings (2 weeks before excisional biopsy). On the T1-weighted axial image (A), the bilateral orbital mass appeared as an isosignal intensity with gray matter of the brain. T2-weighted axial image with fat suppressed image (B) shows the bilateral orbital mass with central low signal intensity. Right (C) and left (D) postcontrast T1-weighted sagittal images demonstrate that elongated extraconal masses (white arrows) in the inferior aspect of both orbit, prominent in the right orbit. The masses with homogeneous low internal signal intensity and higher signal intensity in the peripheral rim (black arrow) are noted.
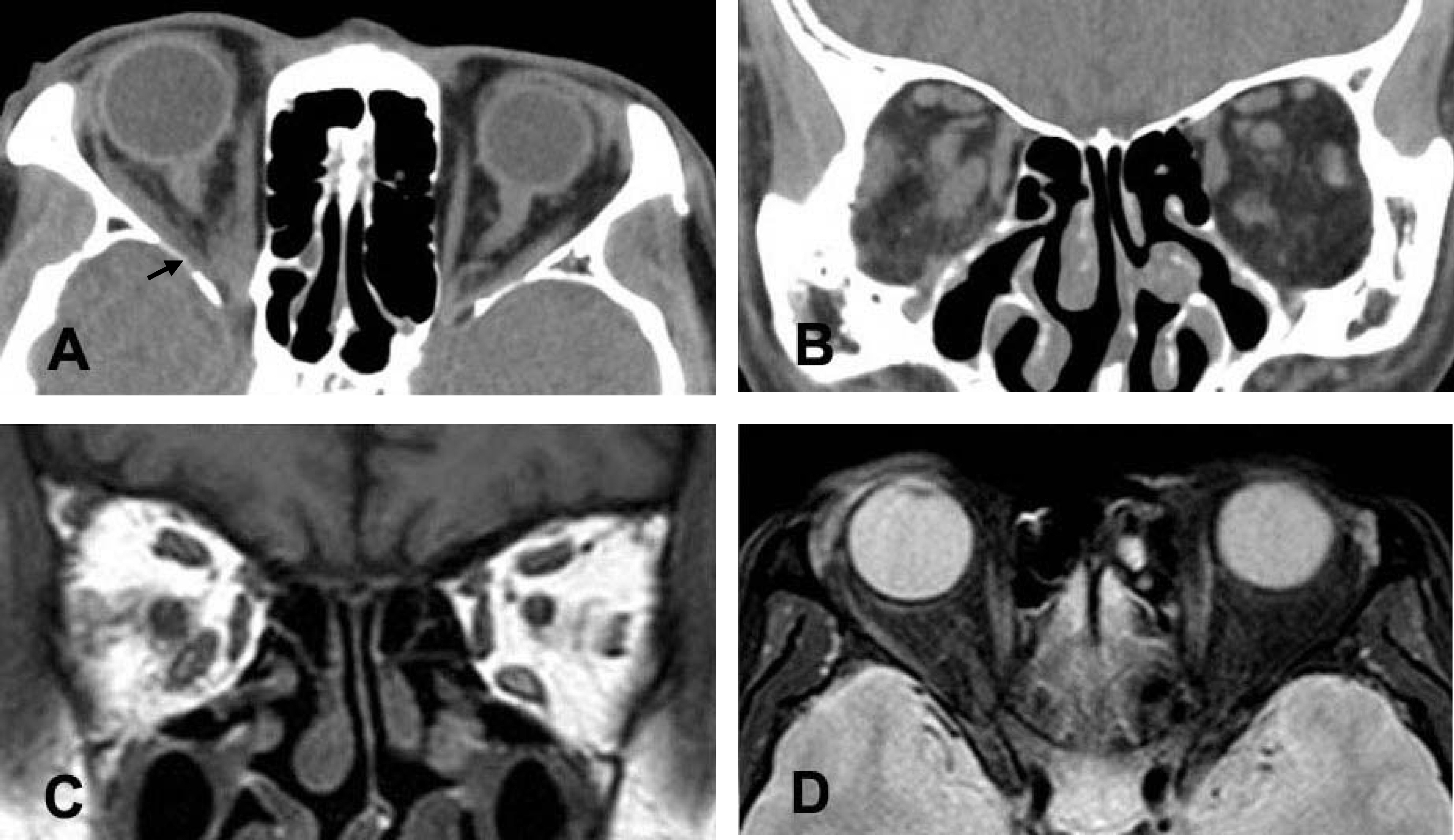
Figure 3. Post-operative follow-up CT (2 hours after excisional biopsy) and MRI (1 day after excisional biopsy) findings. As compared to the previous CT, images reveal marked interval reduction of bilateral orbital masses. Mild swelling of the right inferior rectus muscle is noted and it was regarded as a result of operation. Insignificant residual mass-like lesion (black arrow) in the far posterior aspect of the inferior orbits along the inferior rectus muscles can be seen. (A, B) T1 weighted coronal image (C) and T2 weighted axial with fat suppression image (D) show only mild thickening along inferior rectus muscle and there is no round mass in both orbits which was seen in pre-operative MRI images.
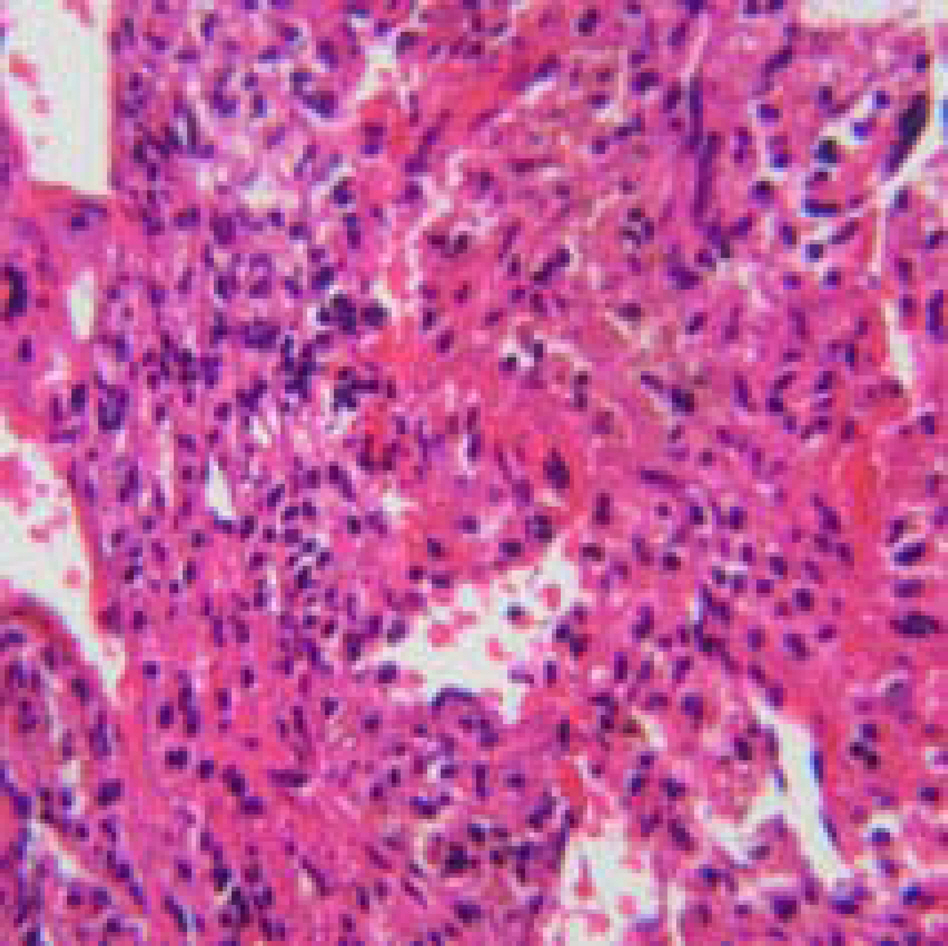
Figure 4. Mild non-specific inflammation with fibrosis (hematoxylin-eosin, ×200). The right orbit.
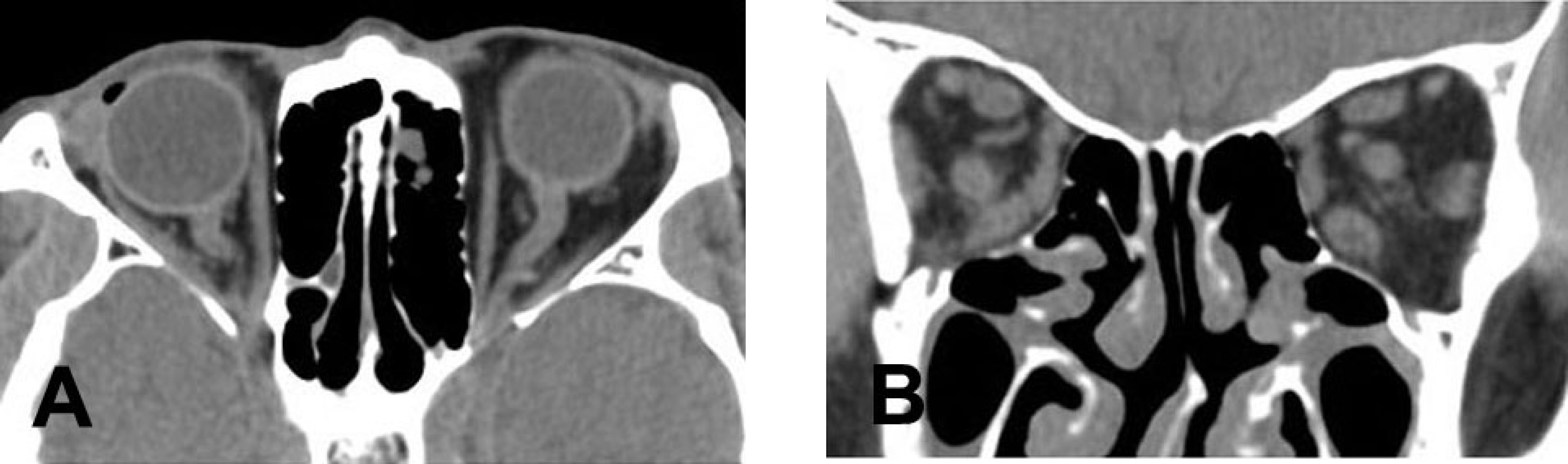
Figure 5. Orbital CT findings at 3 months after diagnosis. On axial and coronal views, tumor-like lesion of both orbits are not noted anymore.
Reference
-
References
1. Birch-Hirschfeld A. Zur Daignostik und Pathologie der Orbital-tumoren. Ber Dtsch Ophthalmol Ges. 1905; 32:127–35.2. Rootman J, McCarthy M, White V, et al. Idiopathic sclerosing inflammation of the orbit. A distinct clinicopathologic entity. Ophthalmology. 1994; 101:570–84.3. Gunalp I, Gunduz K, Yazar Z. Idiopathic orbital inflammatory disease. Acta Ophthalmol Scand. 1996; 74:191–3.4. Demirci H, Shields CL, Shields JA, et al. Orbital tumors in the older adult population. Ophthalmology. 2002; 109:243–8.
Article5. Levine MR, Kaye L, Mair S, Bates J. Multifocal fibrosis. Report of a case of bilateral idiopathic sclerosing pseudotumor and retroperitoneal fibrosis. Arch Ophthalmol. 1993; 111:841–3.6. Kim SH, Sun DY, Kim YD. Clinical characteristics of sclerosing pseudotumor of the orbit. J Korean Ophthalmol Soc. 2000; 41:2157–67.7. Wojno TH, Grossniklaus H. Inflammatory pseudotumor of the eyelid. Ophthal Plast Reconstr Surg. 1995; 11:125–30.
Article8. Rose AG, McCormick S, Cooper K, Titus JL. Inflammatory pseudotumor (plasma cell granuloma) of the heart. Arch Pathol Lab Med. 1996; 120:549–54.9. Mombaerts I, Goldschmeding R, Schlingemann RO, Koornneef L. Clinical pathological review. What is orbital pseudotumor? Surv Ophthalmol. 1996; 41:66–78.10. Devron HC, Theodore M. Orbital Pseudotumor. Fine-needle aspiration biopsy and response to therapy. Ophthalmology. 1993; 100:1702–10.11. Moseley IF, Wright JE. Orbital pseudotumor. Clin Radiol. 1992; 45:67–8.12. Hyun GH, Han SK. Atypical inflammatory orbital pseudotumor with acute pneumonic infiltration. J Korean Ophthalmol Soc. 2001; 42:1798–802.13. Andrade DM, Martins SJ, Paz O, et al. Inflammatory pseudotumor : A diagnostic dilemma. Eur J Intern Med. 2006; 17:514–6.14. Mombaerts I, Schlingemann RO, Goldschmeding R, et al. Are systemic corticosteroids useful in the management of orbital pseudotumors? Ophthalmology. 1996; 103:521–8.
Article15. Lee H, Kim SJ, Lee SY. Classification and treatment efficacy of orbital pseudotumor. J Korean Ophthalmol Soc. 2001; 42:1647–54.16. Maurer I, Zierz S. Recurrent orbital myositis: report of a familial incidence. Arch Neurol. 1999; 56:1407–9.17. Kert G, Clement CI, O'Donell BA. Clinical case notes. Orbital lymphoid tumor located within an extraocular muscle. Clin Experiment Ophthalmol. 2004; 32:651–5.18. Levy S, Sauvanet A, Diebold MD, et al. Spontaneous regression of inflammatory pseudotumor of the liver presenting as an obstructing malignant biliary tumor. Gastrointest Endosc. 2001; 53:371–4.19. Akansel G, Hendrix L, Erickson BA, et al. MRI patterns in orbital malignant lymphoma and atypical lymphocytic infiltrates. Eur J Radiol. 2005; 53:175–81.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Regression of Inflarmmatory Pseudotumor of the Liver by Conservative Therapy
- A Case of Osteosarcoma Developed in a Patient of Untreated Bilateral Retinoblastoma
- A Case of Orbital Pseudotumor
- Ocular Protrusion and Spontaneous Regression in Bilateral Retinoblastomas
- A Case of Inflammatory Pseudotumor Cerebri and Nasal Septum
