Diagnosis of Right Ventricular Vegetation on Late Gadolinium-Enhanced MR Imaging in a Pediatric Patient after Repair of a Ventricular Septal Defect
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Seoul Hospital, Seoul, Korea.
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yhchoe@skku.edu
- 3HVSI Imaging Center, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Cardiology, Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2327423
- DOI: http://doi.org/10.13104/imri.2016.20.2.114
Abstract
- We report a case of vegetation in a 4-year-old female with infective endocarditis, diagnosed by late gadolinium-enhanced (LGE) cardiovascular magnetic resonance (CMR) imaging. The patient had a history of primary closure for ventricular septal defect and presented with mild febrile sensation. No remarkable clinical symptoms or laboratory findings were noted; however, transthoracic echocardiography demonstrated a 14 mm highly mobile homogeneous mass in the right ventricle. On LGE CMR imaging, the mass showed marginal rim enhancement, which suggested the diagnosis of vegetation rather than thrombus. The extracellular volume fraction (≥ 42%) of the lesion was higher than that of normal myocardium. Based on the patient's clinical history of congenital heart disease and pathologic confirmation of the lesion, a diagnosis of infective endocarditis with vegetation was made.
Keyword
MeSH Terms
Figure
-
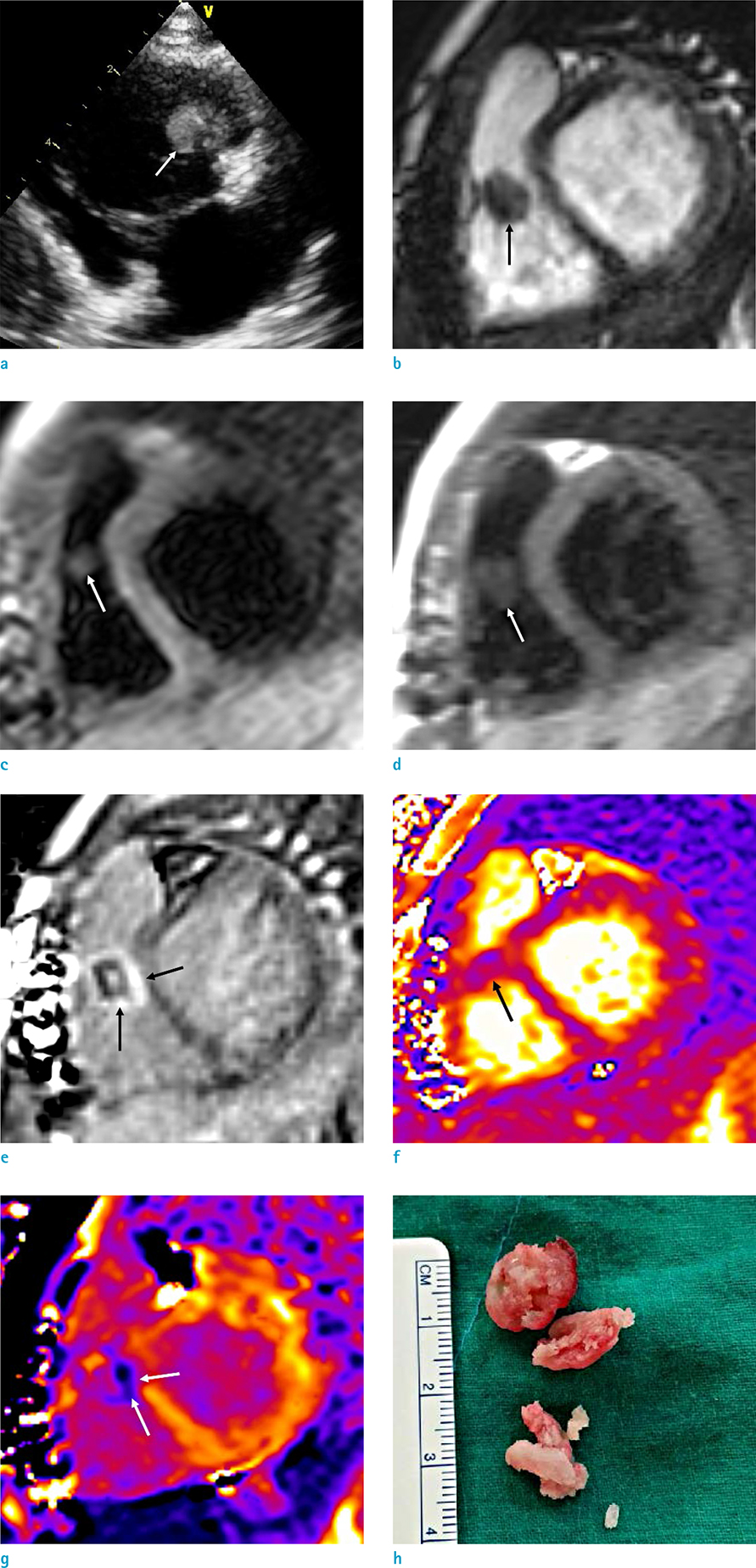
Fig. 1 A 4-year-old female with a vegetation in the right ventricle (RV). (a) Initial transthoracic echocardiography shows a14 × 11 mm-sized highly mobile homogeneous mass (arrowhead) in RV, which is attached to the ventricular septal defect primary closure site. (b-e) CMR (b), 8 days after initial the echocardiography. The mass (white arrows) is seen in the RV, attached to the anterior wall on a short-axis-view cine MR image and shows iso-signal intensity as compared with the myocardium on T2-weighted (c) and T1-weighted (d) images. Late gadolinium-enhanced image in a short-axis view (e) demonstrates marginal rim enhancements (black arrows). (f, g) A T2 map (f) and postcontrast-T1 map image (g) show that the T2 relaxation time of the lesion is similar to that of normal left ventricular myocardium and that peripheral components (arrows) of the vegetation show lower T1 values than the myocardium. (h) Resected specimen shows a soft, round, encapsulated, and whitish mass consisting of granular tissue.
Reference
-
1. Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009; 30:2369–2413.2. Dursun M, Yilmaz S, Yilmaz E, et al. The utility of cardiac MRI in diagnosis of infective endocarditis: preliminary results. Diagn Interv Radiol. 2015; 21:28–33.3. Thuny F, Grisoli D, Cautela J, Riberi A, Raoult D, Habib G. Infective endocarditis: prevention, diagnosis, and management. Can J Cardiol. 2014; 30:1046–1057.4. Bae JM, Choe YH, Hwang HW, et al. Tumor-mimicking large vegetation attached to the tricuspid valve without predisposing factors: a case report on CT and echocardiographic findings. J Korean Soc Radiol. 2015; 73:269–273.5. Knirsch W, Nadal D. Infective endocarditis in congenital heart disease. Eur J Pediatr. 2011; 170:1111–1127.6. Elder RW, Baltimore RS. The changing epidemiology of pediatric endocarditis. Infect Dis Clin North Am. 2015; 29:513–524.7. Bruun NE, Habib G, Thuny F, Sogaard P. Cardiac imaging in infectious endocarditis. Eur Heart J. 2014; 35:624–632.8. Sparrow PJ, Kurian JB, Jones TR, Sivananthan MU. MR imaging of cardiac tumors. Radiographics. 2005; 25:1255–1276.9. Dursun M, Yilmaz S, Ali Sayin O, et al. A rare cause of delayed contrast enhancement on cardiac magnetic resonance imaging: infective endocarditis. J Comput Assist Tomogr. 2005; 29:709–711.10. Sverdlov AL, Taylor K, Elkington AG, Zeitz CJ, Beltrame JF. Images in cardiovascular medicine. Cardiac magnetic resonance imaging identifies the elusive perivalvular abscess. Circulation. 2008; 118:e1–e3.11. Ryu SY, Kim HJ, Kim SM, Park SJ, Choe YH. Detection of perivalvular abscess with late gadolinium-enhanced MR imaging in a patient with infective endocarditis. Investig Magn Reson Imaging. 2016; 20:75–79.12. Germain P, El Ghannudi S, Jeung MY, et al. Native T1 mapping of the heart - a pictorial review. Clin Med Insights Cardiol. 2014; 8:1–11.13. Saba SG, Bandettini PW, Shanbhag SM, Spottiswoode BS, Kellman P, Arai AE. Characterization of cardiac masses with T1 mapping. J Cardiovasc Magn Reson. 2015; 17:Suppl 1. Q32.14. Fontana M, White SK, Banypersad SM, et al. Comparison of T1 mapping techniques for ECV quantification. Histological validation and reproducibility of ShMOLLI versus multibreath-hold T1 quantification equilibrium contrast CMR. J Cardiovasc Magn Reson. 2012; 14:88.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The muscular ventricular septal defect and multiple ventricular septal defects in some congenital heart diseases
- Pulmonary Thromboembolism and Infarction Caused by Right-Sided Infective Endocarditis in a Patient with Ventricular Septal Defect
- A Case Report of Ventricular Septal Defect with Bacterial Endocarditis and Pulmonic Valve Vegetation
- Reoperation of Postinfarction VSD
- A Case of Traumatic Ventricular Septal Defect Secondary to Nonpenetrating Chest Trauma
