J Korean Surg Soc.
2010 Sep;79(3):207-214.
Diagnosis of Acute Appendicitis Using Scoring System: Compared with the Alvarado Score
- Affiliations
-
- 1Department of Surgery, Hana Hospital, Cheongju, Korea.
- 2Department of Surgery, Chungbuk National University Hospital, Cheongju, Korea. colon@chungbuk.ac.kr
- 3Department of Surgery, Cheongju Medical Center, Cheongju, Korea.
- 4Department of Surgery, Cheongju St. Mary's Hospital, Cheongju, Korea.
- 5Department of Surgery, Hyosung Hospital, Cheongju, Korea.
Abstract
- PURPOSE
This study evaluated the usefulness of a new scoring system in diagnosing acute appendicitis which expresses the patient's symptoms, physical examination, and laboratory findings more clearly and objectively.
METHODS
A prospective study was conducted with 314 patients who were hospitalized with suspicion of acute appendicitis. After analyzing the symptoms, physical examination, and laboratory findings, 10 meaningful variables were selected, each of which were scored separately. The diagnostic value of the new scoring system was evaluated, and analyzed in comparison to the preexisting Alvarado score.
RESULTS
Ten variables including vomiting, migration pain, fever, Dunphy's sign, Rovsing's sign, tenderness, rebound tenderness, increased white blood cell counts, increased neutrophil proportion, and increased CRP levels were associated with acute appendicitis. The new scoring system is developed by applying 1 point for each variable, with a total score of 10 points. In the new scoring system, a score above 5 points had sensitivity of 0.75, specificity of 0.73, positive predictive value of 0.92, and diagnostic accuracy of 0.71. The area under the receiver operating characteristic curve was 0.80, which is larger than 0.72 of the preexisting Alvarado score, and thus has a higher diagnostic accuracy. As acute appendicitis progresses, the average score tends to become significantly higher (P=0.001).
CONCLUSION
The new scoring system, which objectively reflects the clinical variables of the patient's symptoms, physical examination and laboratory findings, will be useful in accurately diagnosing acute appendicitis and in quickly deciding a therapeutic policy in patients with right lower abdominal pain.
MeSH Terms
Figure
-
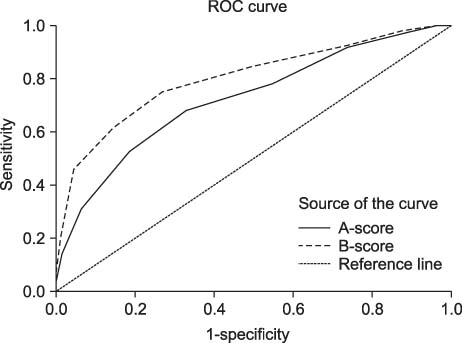
Fig. 1 Comparison of receiver operating characteristic (ROC) curves of Alvarado score (A-score) and new scoring system (B-score). Area under curve of B-score is larger than that of A-score.
Reference
-
1. Jones PF. Suspected acute appendicitis: trends in management over 30 years. Br J Surg. 2001. 88:1570–1577.2. Andersson R, Hugander A, Thulin A, Nyström PO, Olaison G. Indications for operation in suspected appendicitis and incidence of perforation. BMJ. 1994. 308:107–110.3. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990. 132:910–925.4. Lewis FR, Holcroft JW, Boey J, Dunphy E. Appendicitis. A critical review of diagnosis and treatment in 1,000 cases. Arch Surg. 1975. 110:677–684.5. Gupta H, Dupuy DE. Advances in imaging of the acute abdomen. Surg Clin North Am. 1997. 77:1245–1263.6. Terasawa T, Blackmore CC, Bent S, Kohlwes RJ. Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Ann Intern Med. 2004. 141:537–546.7. Heller MB, Skolnick ML. Ultrasound documentation of spontaneously resolving appendicitis. Am J Emerg Med. 1993. 11:51–53.8. Andersson RE. Resolving appendicitis is common: further evidence. Ann Surg. 2008. 247:553.9. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986. 15:557–564.10. Andersson RE, Hugander A, Ravn H, Offenbartl K, Ghazi SH, Nyström PO, et al. Repeated clinical and laboratory examinations in patients with an equivocal diagnosis of appendicitis. World J Surg. 2000. 24:479–485.11. Teicher I, Landa B, Cohen M, Kabnick LS, Wise L. Scoring system to aid in diagnoses of appendicitis. Ann Surg. 1983. 198:753–759.12. Owen TD, Williams H, Stiff G, Jenkinson LR, Rees BI. Evaluation of the Alvarado score in acute appendicitis. J R Soc Med. 1992. 85:87–88.13. Sun JS, Noh HW, Min YG, Lee JH, Kim JK, Park KJ, et al. Receiver operating characteristic analysis of the diagnostic performance of a computed tomographic examination and the Alvarado score for diagnosing acute appendicitis: emphasis on age and sex of the patients. J Comput Assist Tomogr. 2008. 32:386–391.14. Perez J, Barone JE, Wilbanks TO, Jorgensson D, Corvo PR. Liberal use of computed tomography scanning does not improve diagnostic accuracy in appendicitis. Am J Surg. 2003. 185:194–197.15. Chan MY, Teo BS, Ng BL. The Alvarado score and acute appendicitis. Ann Acad Med Singapore. 2001. 30:510–512.16. Subotić AM, Sijacki AD, Dugalić VD, Antić AA, Vuković GM, Vukojević VS, et al. Evaluation of the Alvarado score in the diagnosis of acute appendicitis. Acta Chir Iugosl. 2008. 55:55–61.17. Jahn H, Mathiesen FK, Neckelmann K, Hovendal CP, Bellstrøm T, Gottrup F. Comparison of clinical judgment and diagnostic ultrasonography in the diagnosis of acute appendicitis: experience with a score-aided diagnosis. Eur J Surg. 1997. 163:433–443.18. Andersson M, Andersson RE. The appendicitis inflammatory response score: a tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J Surg. 2008. 32:1843–1849.19. Wu HP, Huang CY, Chang YJ, Chou CC, Lin CY. Use of changes over time in serum inflammatory parameters in patients with equivocal appendicitis. Surgery. 2006. 139:789–796.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of Alvarado Score in Patients with Suspected Appendicitis
- The Effectiveness of a Repeatedly Checked Alvarado Score as a Screening Tool for Acute Appendicitis
- Diagnostic Efficacy of the Alvarado Score according to Age in Acute Appendicitis
- Which One is Better? Comparison of the Acute Inflammatory Response, Raja Isteri Pengiran Anak Saleha Appendicitis and Alvarado Scoring Systems
- Usefulness of a Alvarado Scoring System for the Diagnosis of Acute Appendicitis in Children
