J Korean Soc Spine Surg.
2004 Dec;11(4):278-284.
Comparative Analysis of Unstable Burst Fracture According to the Methodology of Surgical Treatment
- Affiliations
-
- 1Department of Orthopedic Surgery, Guri Hospital, Hanyang University College of Medicine, Guri, Korea. hyparkys@hanyang.ac.kr
- 2Department of Orthopedic Surgery, Hanyang University College of Medicine, Seoul, Korea.
Abstract
- STUDY DESIGN: A retrospective analysis of the results of various methodologies for the surgical treatment of an unstable burst fracture with posterior column injuries.
OBJECTIVES
To compare the radiological and clinical results in unstable burst fractures, treated with various surgical methodologies (anterior, posterior and combined fusion), and to confirm their efficacy. LITERATURE REVIEW SUMMARY: Many authors recommended various surgical methods for the treatment of an unstable burst fracture, and of these, combined fusion is recommended for the preservation of stability.
MATERIALS AND METHODS
A retrospective review of results was carried out on 22 patients, confirmed with an unstable burst fracture associated with a posterior column injury, between Nov. 1996 and Mar. 2003. The preoperative plane x-ray, CT and MRI, and the last postoperative follow up plane X-ray and CT, in 22 unstable burst fracture patients, were reviewed. The authors looked for laminar fracture, facet injury and inter-spinous widening in the plane x-ray, canal compromise on the CT, and a posterior ligament injury and dural tear on the MRI. The neurological injury was evaluated using the Bardford and McBride criteria and the clinical result with the Denis' pain and work scale.
RESULTS
In the anterior fusion group, the radiological findings showed 3 laminar fractures, 2 facet injuries, 7 inter-spinous widening and 8 posterior ligament injuries. In the posterior fusion group, they showed 5 laminar fractures, 4 facet injuries, 5 inter-spinous widening and 5 posterior ligament injuries. In the combined fusion group, they showed 5 laminar fractures, 4 facet injuries, 4 inter-spinous widening and 5 posterior ligament injuries. The average canal compromise was 54.3% in cases of anterior fusion, 20.9% of posterior fusion and 74% of the combined fusion groups. A dural tear was found in 1 each of the anterior and posterior and 4 of the combined group. From the clinical results, improvements of the neurology in the anterior, posterior and combined groups were 2.0, 1.7 and 1.3 degrees, respectively. From the Denis' pain & work scale better than good degrees were shown in 3 of the anterior, 4 of the posterior and 2 of the combined groups.
CONCLUSIONS
In conclusion, there were no differences in the improvements of the neurology and clinical results according to the surgical methodology employed. However, the use of combined fusion is recommended for the preservation of stability in an unstable burst fracture with combined posterior ligament and bony injuries as well as with severe canal compromise.
MeSH Terms
Figure
-

Fig. 1. In simple radiographs, it shows widening of interpedicular distance, collapse of anterior and middle column and interspinous widening.

Fig. 2. The CT image shows over 60% encroachment of spinal canal and laminar fracture.

Fig. 3. In MRI, it shows injury of posterior ligament complex.
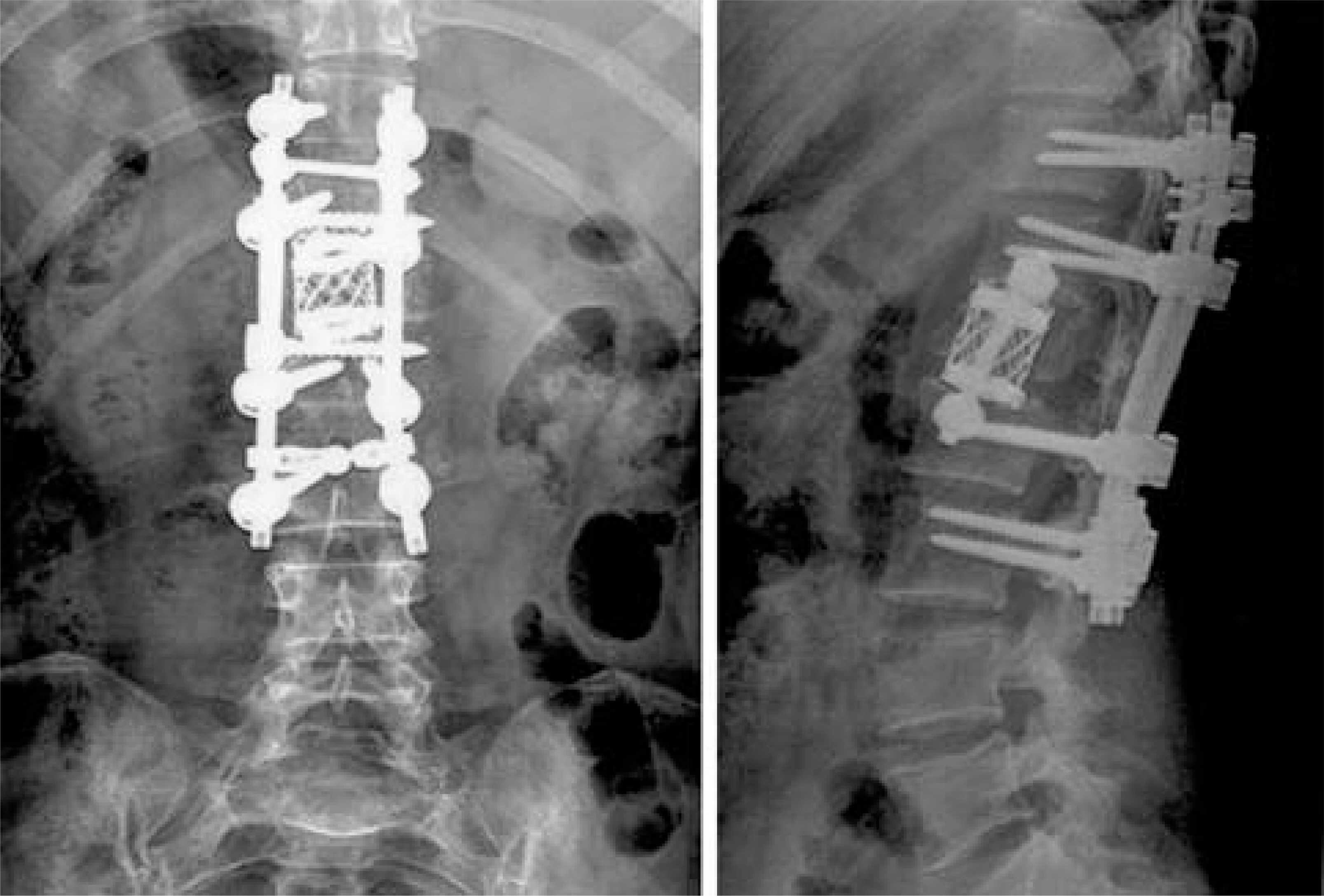
Fig. 4. In follow-up radiopgraphs, it shows circumferential fusion of the unstable burst fracture.
Reference
-
1). Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma: Clin Orthop. 1984. 65–76.2). McAfee PC, Yuan HA, Lasda NA. The unstable burst fracture: Spine. 1982; 7:365–373.3). Gertzbein SD, Court-Brown CM, Marks P, et al. The neurological outcome following surgery for spinal fractures: Spine. 1988; 13:641–644.4). Hu SS, Capen DA, Rimoldi RL, Zigler JE. The effect of surgical decompression on neurologic outcome after lumbar fractures: Clin Orthop. 1993. 166–173.5). Bradford DS, McBride GG. Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits: Clin Orthop. 1987. 201–216.6). McAfee PC, Bohlman HH, Yuan HA. Anterior decompression of traumatic thoracolumbar fractures with incomplete neurological deficit using a retroperitoneal approach: J Bone Joint Surg Am. 1985; 67:89–104.7). Okuyama K, Abe E, Chiba M, Ishikawa N, Sato K. Outcome of anterior decompression and stabilization for thoracolumbar unstable burst fractures in the absence of neurologic deficits: Spine. 1996; 21:620–625.8). Hardaker WT Jr, Cook WA Jr, Friedman AH, Fitch RD. Bilateral transpedicular decompression and Harring -ton rod stabilization in the management of severe thoracolumbar burst fractures: Spine. 1992; 17:162–171.9). Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations: Spine. 1992; 17:S317–324.10). Danisa OA, Shaffrey CI, Jane JA, et al. Su r g i cal approaches for the correction of unstable thoracolumbar burst fractures: a retrospective analysis of treatment outcomes: J Neurosurg. 1995; 83:977–983.11). Grob D, Scheier HJ, Dvorak J, Siegrist H, Rubeli M, Joller R. Circumferential fusion of the lumbar and lumbosacral spine: Arch Orthop Trauma Surg. 1991; 111:20–25.12). Gertzbein SD, Court-Brown CM, Jacobs RR, et al. Decompression and circumferential stabilization of unstable spinal fractures: Spine. 1988; 13:892–895.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Crush-Cleavage Fracture in Thoracolumbar and Lumbar Spine: Comparative Study with Type B Burst Fracture
- Are “Unstable” Burst Fractures Really Unstable?
- One Stage Decompression and Circumferential Stabilization by Posterior Approach in the Unstable Burst Fracture of Thoracolumbar and Lumbar Spine
- Comparative Study of Radiologic Changes after Conservative Treatment in Compression fracture and Stable Bursting Fracture of Thoracolumbar Spine
- Assessment of Operative Reduction in Thoracolumbar and Lumbar Spine Fractures
