A Case of Pulmonary Siderosis Mimicking Metastatic Lung Cancer
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon, Korea. swpark@schmc.ac.kr
- 2Department of Radiology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 3Department of Pathology, Soonchunhyang University College of Medicine, Bucheon, Korea.
Abstract
- Pulmonary siderosis is a pneumoconiosis caused by chronic iron inhalation. A diagnosis of pulmonary siderosis is based on a patient history of iron inhalation, on chest radiographic findings, and on accumulation of iron oxide in macrophages within the lung. A typical radiographic finding of pulmonary siderosis includes ill-defined micronodules that are diffusely distributed in the lung. We experienced a 52-year-woman with a 1.3x1.5-cm mass in the left upper lobe with multiple nodules in both lungs. Because the radiographic findings were atypical, we conducted a video-assisted thorascopic lung biopsy procedure to exclude the diagnosis of metastatic lung cancer. After confirming iron deposition in the lung tissue and knowing the patient's occupational history of welding iron, we concluded that this was a case of pulmonary siderosis.
Keyword
MeSH Terms
Figure
-
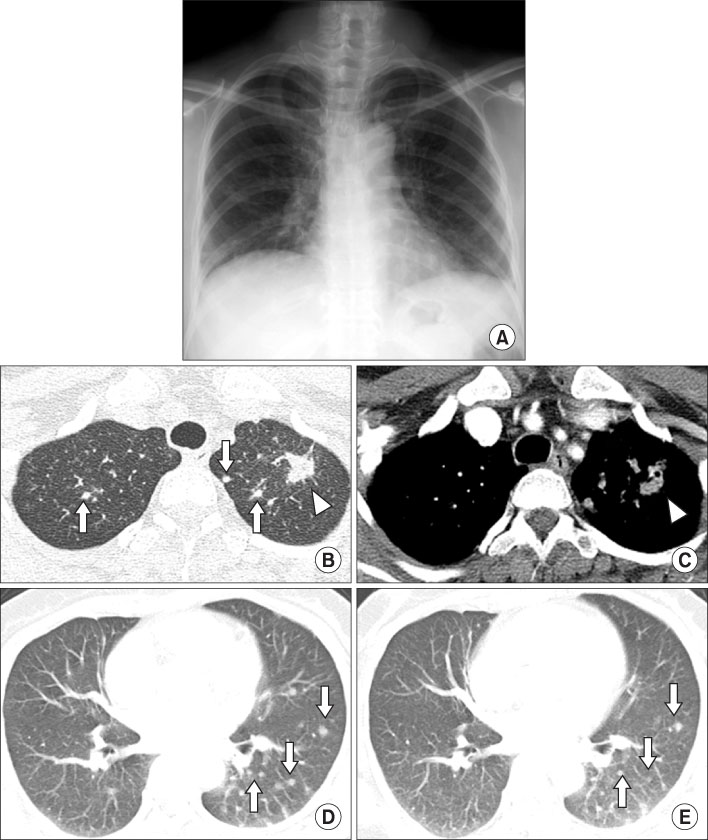
Figure 1 (A) Chest PA shows multiple ill defined irregular nodules in both lungs. (B) Chest CT scan with lung window shows 1.3×1.5 cm sized irregular large nodule (arrowhead) in left upper lobe and multiple round nodules (arrows) in both upper lobes. (C) Chest CT scan with mediastinal window shows 1.3×1.5 cm sized irregular enhancing nodule (arrowhead) in left upper lobe. (D) Chest CT scan with lung window reveals multiple small round nodules (arrows) in left upper lobe and left lower lobe. (E) Follow-up chest CT scan after 4 months shows no interval change of multiple small nodules (arrows).
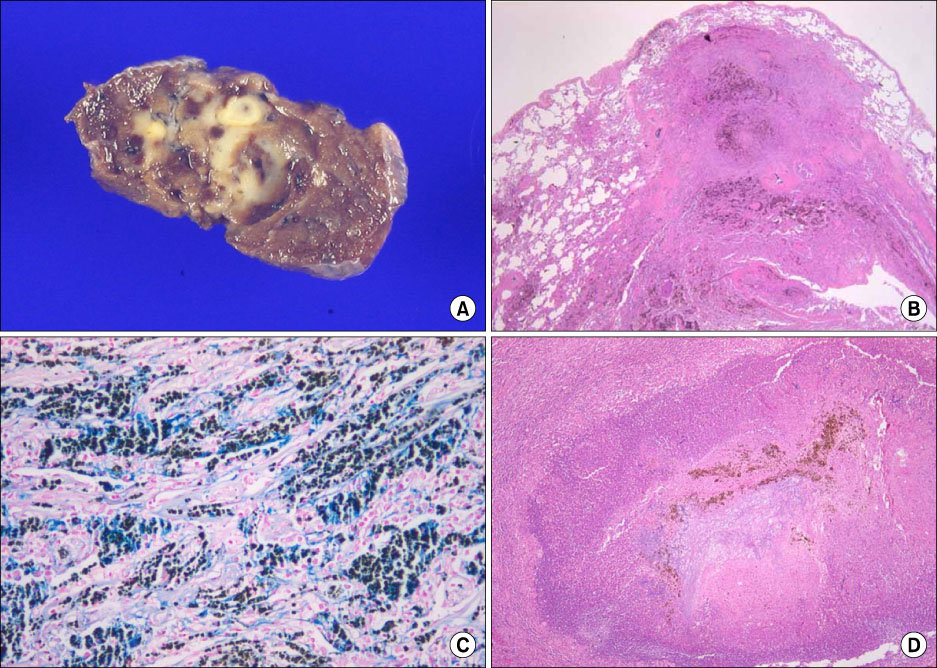
Figure 2 (A) Gross photograph shows ill-defined grayish yellow nodular lesion. (B) Inflammatory fibrotic nodules with brown pigmentation (H&E stain, ×10). (C) Numerous macrophages with bright blue cytoplasmic pigmentation (Prussian blue stain, ×200). (D) Abscess with central colonizing aspergillosis (H&E stain, ×40).
Reference
-
1. Attfield MD, Ross DS. Radiological abnormalities in electric-arc welders. Br J Ind Med. 1978. 35:117–122.2. Lee CU, Cho GY, Kim SC, Pae KT, Kim YW, Yun IG. The epidemiologial study on the welders' pneumoconiosis among shipyard welders in Pusan area. Korean J Prev Med. 1989. 22:153–161.3. Guidotti TL, Abraham JL, DeNee PB, Smith JR. Arc welders' pneumoconiosis: application of advanced scanning electron microscopy. Arch Environ Health. 1978. 33:117–124.4. Billings CG, Howard P. Occupational siderosis and welders' lung: a review. Monaldi Arch Chest Dis. 1993. 48:304–314.5. McCormick LM, Goddard M, Mahadeva R. Pulmonary fibrosis secondary to siderosis causing symptomatic respiratory disease: a case report. J Med Case Reports. 2008. 2:257.6. Chong S, Lee KS, Chung MJ, Han J, Kwon OJ, Kim TS. Pneumoconiosis: comparison of imaging and pathologic findings. Radiographics. 2006. 26:59–77.7. Han D, Goo JM, Im JG, Lee KS, Park DM, Park SH. Thin-section CT findings of arc-welders' pneumoconiosis. Korean J Radiol. 2000. 1:79–83.8. Shipley RT. The 1980 ILO classification of radiographs of the pneumoconioses. Radiol Clin North Am. 1992. 30:1135–1145.9. Park DY, Hwang JH, Kang BS, Chung CS, Kim WJ. Comparision of chest radiographs and pulmonary function in coal workers' pneumoconiosis and welders' lung. Tuberc Respir Dis. 1995. 42:713–722.10. Kinoshita M, Hanzawa S, Momiki S, Sasaki K, Hashizume I, Kasamatsu N, et al. A case of pneumoconiosis (welder's lung) suspected to be lung cancer. Nihon Kyobu Shikkan Gakkai Zasshi. 1997. 35:1124–1131.11. Antonini JM, Lewis AB, Roberts JR, Whaley DA. Pulmonary effects of welding fumes: review of worker and experimental animal studies. Am J Ind Med. 2003. 43:350–360.12. Doherty MJ, Healy M, Richardson SG, Fisher NC. Total body iron overload in welder's siderosis. Occup Environ Med. 2004. 61:82–85.13. Yamada G, Igarashi T, Sonoda H, Morita S, Suzuki K, Yoshida Y, et al. Use of bronchopulmonary lavage for eliminating inhaled fume particles from a patient with arc welder's lung. Intern Med. 1998. 37:962–964.14. Han MS, Kim DI, Cha YS, Kook JH, Yoon KH, Kim JS, et al. A case of pulmonary siderosis. Korean J Med. 1997. 53:731–735.15. Kim EA, Bang BU, Kim L, Ryu JS, Kwak SM, Lee HL, et al. A case of pulmonary siderosis confirmed by bronchoalveolar lavage and transbronchial lung biopsy. Tuberc Respir Dis. 2004. 57:476–479.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Siderosis
- A case of pulmonary siderosis confirmed by bronchoalveolar lavage and transbronchial lung biopsy
- Primary Pulmonary Meningioma Mimicking Lung Metastasis: A Case Report
- A Case of Welder's Lung Disease and Concurred Non-Tuberculotic Mycobacterial Infection Confirmed with Thoracoscopic Lung Biopsy
- Metastatic Lung Nodule of Thyroid Papillary Carcinoma, Mimicking Primary Lung Cancer
