Stone Attenuation Value and Cross-Sectional Area on Computed Tomography Predict the Success of Shock Wave Lithotripsy
- Affiliations
-
- 1Department of Urology, Juntendo University, Tokyo, Japan. michio-t@juntendo.ac.jp
- 2Department of Urology, Juntendo University Urayasu Hospital, Chiba, Japan.
- 3Department of Urology, Juntendo University Nerima Hospital, Tokyo, Japan.
- 4Department of Urology, Juntendo University Shizuoka Hospital, Tokyo, Japan.
- 5Department of Urology, Koshigaya Municipal Hospital, Saitama, Japan.
Abstract
- PURPOSE
To identify the parameters on noncontrast computed tomography (NCCT) that best predict the success of shock wave lithotripsy (SWL).
MATERIALS AND METHODS
We reviewed the records of 75 patients who underwent SWL for urinary calculi measuring 5 to 20 mm. Using NCCT images, we estimated the largest stone cross-sectional area and contoured the inner edge of the stone. Clinical outcome was classified as successful (stone-free or <4 mm in diameter) or failed (stone fragments, > or =4 mm). The impact of preoperative parameters was evaluated by univariate and multivariate analysis.
RESULTS
The overall success rate was 73.3%. Average stone attenuation value, stone length, and stone cross-sectional area in the success and failure groups were 627.4+/-166.5 HU (Hounsfield unit) vs. 788.1+/-233.9 HU (p=0.002), 11.7+/-3.8 mm vs. 14.2+/-3.6 mm (p=0.015), and 0.31+/-0.17 cm2 vs. 0.57+/-0.41 cm2 (p<0.001), respectively. In the multivariate analysis, stone attenuation value was the only independent predictor of SWL success (p=0.023), although stone cross-sectional area had a tendency to be associated with SWL success (p=0.053). Patients were then classified into four groups by using cutoff values of 780 HU for stone attenuation value and 0.4 cm2 for cross-sectional area. By use of these cutoff values, the group with a low stone attenuation value and a low cross-sectional area was more than 11.6 times as likely to have a successful result on SWL as were all other groups (odds ratio, 11.6; 95% confidence interval, 3.9 to 54.7; p<0.001).
CONCLUSIONS
Stone attenuation value and stone cross-sectional area are good predictors of extracorporeal SWL outcome.
Figure
-
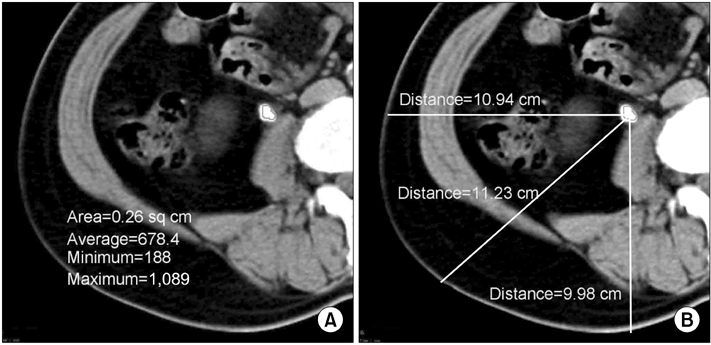
FIG. 1 Measurement technique. (A) Stone area and stone attenuation values were calculated by using noncontrast computed tomography images archived to a POP-Net Server (Image ONE Co.). (B) Stone-to-skin distance was defined as the average of measurements taken at 0°, 45°, and 90°.
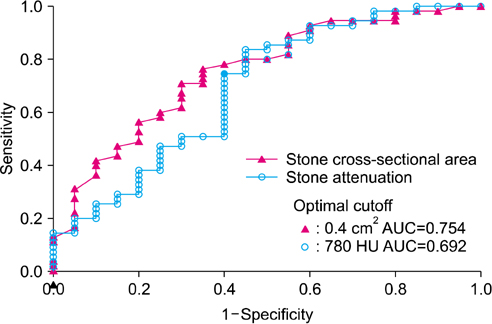
FIG. 2 Receiver operating characteristic (ROC) curve for stone attenuation and stone cross-sectional area of shock wave lithotripsy. AUC, area under the curve; HU, Hounsfield unit.
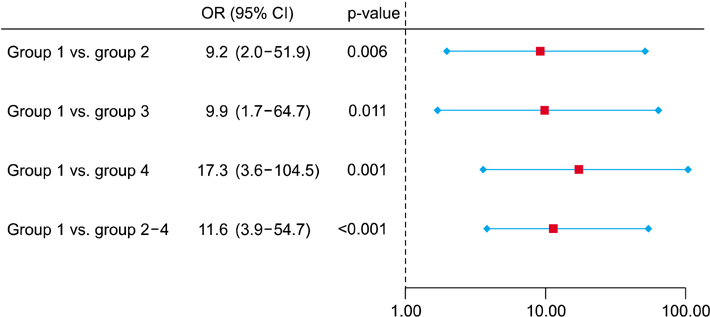
FIG. 3 Odds ratios for successful shock wave lithotripsy outcome according to stone attenuation value and cross-sectional area. Group 1, attenuation ≤780 HU (Hounsfield unit) and cross-sectional area ≤0.4 cm2; group 2, ≤780 HU and >0.4 cm2; group 3, >780 HU and ≤0.4 cm2; and group 4, >780 HU and >0.4 cm2. OR, odds ratio; CI, confidence interval.
Reference
-
1. Preminger GM, Tiselius HG, Assimos DG, Alken P, Buck AC, Gallucci M, et al. 2007 Guideline for the management of ureteral calculi. Eur Urol. 2007. 52:1610–1631.2. Kijvikai K, Haleblian GE, Preminger GM, de la Rosette J. Shock wave lithotripsy or ureteroscopy for the management of proximal ureteral calculi: an old discussion revisited. J Urol. 2007. 178(4 Pt 1):1157–1163.3. Joseph P, Mandal AK, Singh SK, Mandal P, Sankhwar SN, Sharma SK. Computerized tomography attenuation value of renal calculus: can it predict successful fragmentation of the calculus by extracorporeal shock wave lithotripsy? A preliminary study. J Urol. 2002. 167:1968–1971.4. Pareek G, Armenakas NA, Fracchia JA. Hounsfield units on computerized tomography predict stone-free rates after extracorporeal shock wave lithotripsy. J Urol. 2003. 169:1679–1681.5. Pareek G, Armenakas NA, Panagopoulos G, Bruno JJ, Fracchia JA. Extracorporeal shock wave lithotripsy success based on body mass index and Hounsfield units. Urology. 2005. 65:33–36.6. Pareek G, Hedican SP, Lee FT Jr, Nakada SY. Shock wave lithotripsy success determined by skin-to-stone distance on computed tomography. Urology. 2005. 66:941–944.7. Perks AE, Gotto G, Teichman JM. Shock wave lithotripsy correlates with stone density on preoperative computerized tomography. J Urol. 2007. 178(3 Pt 1):912–915.8. Bon D, Dore B, Irani J, Marroncle M, Aubert J. Radiographic prognostic criteria for extracorporeal shock-wave lithotripsy: a study of 485 patients. Urology. 1996. 48:556–560.9. Pfister SA, Deckart A, Laschke S, Dellas S, Otto U, Buitrago C, et al. Unenhanced helical computed tomography vs intravenous urography in patients with acute flank pain: accuracy and economic impact in a randomized prospective trial. Eur Radiol. 2003. 13:2513–2520.10. Eikefjord E, Askildsen JE, Rorvik J. Cost-effectiveness analysis (CEA) of intravenous urography (IVU) and unenhanced multidetector computed tomography (MDCT) for initial investigation of suspected acute ureterolithiasis. Acta Radiol. 2008. 49:222–229.11. Kacker R, Zhao L, Macejko A, Thaxton CS, Stern J, Liu JJ, et al. Radiographic parameters on noncontrast computerized tomography predictive of shock wave lithotripsy success. J Urol. 2008. 179:1866–1871.12. Perks AE, Schuler TD, Lee J, Ghiculete D, Chung DG, D'A Honey RJ, et al. Stone attenuation and skin-to-stone distance on computed tomography predicts for stone fragmentation by shock wave lithotripsy. Urology. 2008. 72:765–769.13. Dretler SP, Polykoff G. Calcium oxalate stone morphology: fine tuning our therapeutic distinctions. J Urol. 1996. 155:828–833.14. Nakada SY, Hoff DG, Attai S, Heisey D, Blankenbaker D, Pozniak M. Determination of stone composition by noncontrast spiral computed tomography in the clinical setting. Urology. 2000. 55:816–819.15. Zarse CA, McAteer JA, Tann M, Sommer AJ, Kim SC, Paterson RF, et al. Helical computed tomography accurately reports urinary stone composition using attenuation values: in vitro verification using high-resolution micro-computed tomography calibrated to fourier transform infrared microspectroscopy. Urology. 2004. 63:828–833.16. Saw KC, McAteer JA, Monga AG, Chua GT, Lingeman JE, Williams JC Jr. Helical CT of urinary calculi: effect of stone composition, stone size, and scan collimation. AJR Am J Roentgenol. 2000. 175:329–332.17. Tiselius HG. How efficient is extracorporeal shockwave lithotripsy with modern lithotripters for removal of ureteral stones? J Endourol. 2008. 22:249–255.18. Lam HS, Lingeman JE, Russo R, Chua GT. Stone surface area determination techniques: a unifying concept of staghorn stone burden assessment. J Urol. 1992. 148(3 Pt 2):1026–1029.19. Yoshida S, Hayashi T, Ikeda J, Yoshinaga A, Ohno R, Ishii N, et al. Role of volume and attenuation value histogram of urinary stone on noncontrast helical computed tomography as predictor of fragility by extracorporeal shock wave lithotripsy. Urology. 2006. 68:33–37.20. Ng CF, Siu DY, Wong A, Goggins W, Chan ES, Wong KT. Development of a scoring system from noncontrast computerized tomography measurements to improve the selection of upper ureteral stone for extracorporeal shock wave lithotripsy. J Urol. 2009. 181:1151–1157.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extracorporeal shock wave lithotripsy of lower caliceal stone
- Clinical Experience of Extracorporeal Shock Wave Lithotripsy for Urinary Calculi
- Evaluating the importance of different computed tomography scan-based factors in predicting the outcome of extracorporeal shock wave lithotripsy for renal stones
- Effects of Extracorporeal Shock Wave Lithortripsy Experimentally Induced Cholelithiasis and Organs in the Dog
- Non-surgical treatment of urinary stone
