Cystoscopic Extraction Technique and External Drainage Rescue of a Failed Attempt to Traverse a Severe Transplanted Ureteral Obstruction
- Affiliations
-
- 1Centre of Medical Interventional Therapy, General Hospital of Jinan Military Command, Jinan, China. sungangmilit@163.com
- 2Department of Urology, Shandong Jiaotong Hospital, Jinan, China.
Abstract
- PURPOSE
The aim of this research was to evaluate the efficacy of the cystoscopic extraction and external drainage techniques for unsuccessful antegrade stenting in transplanted severe ureteral obstruction.
MATERIALS AND METHODS
A total of 26 patients with severe transplanted ureteral obstruction in whom the cystoscopic extraction technique and/or external drainage technique was performed were retrospectively evaluated. After the severe obstruction was successfully traversed, balloon dilatation followed by double-J stent insertion was performed.
RESULTS
Of the 26 patients (male:female, 9:4; mean age, 38.1 years) who underwent failed ureteral stenting with the conventional procedure, 16 patients underwent successful stenting with the cystoscopic extraction technique, and 10 patients underwent successful stenting following external drainage. The mean serum creatinine of the 26 patients before stenting was 42.9 mg/dL (range, 32.7 to 54.1 mg/dL), which decreased to 10.3 mg/dL (range, 8.7 to 11.8 mg/dL) after stenting. The complications of the procedure were lower abdominal pain in 22 patients and gross hematuria in 9 patients. All complications were relieved with medical care within 3 to 5 days after the procedure. No major complications occurred.
CONCLUSIONS
The cystoscopic extraction technique and external drainage technique are safe and useful for traversing a severe transplanted ureteral obstruction after a failed conventional procedure.
Keyword
MeSH Terms
Figure
-
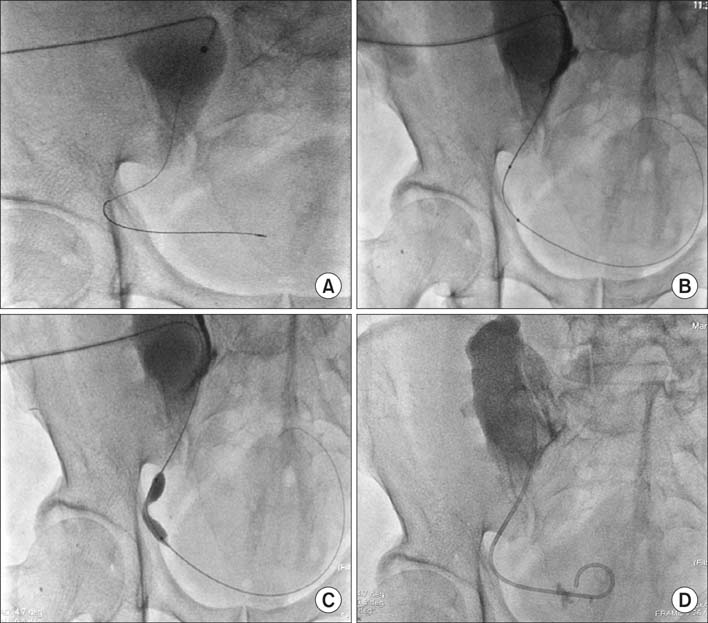
FIG. 1 Medical imaging of digital subtraction angiography: a 58-year-old patient with a transplanted ureteric obstruction. (A) The portion of the guidewire crossing the stricture into the bladder was too short for the catheter to follow it. (B) After the cystoscopic extraction technique, the distal portion of the guidewire was coiled in the bladder following balloon insertion. (C) The notch of the balloon catheter for ureteroplasty showed ureteric stricture. (D) The double-J stent was inserted successfully.
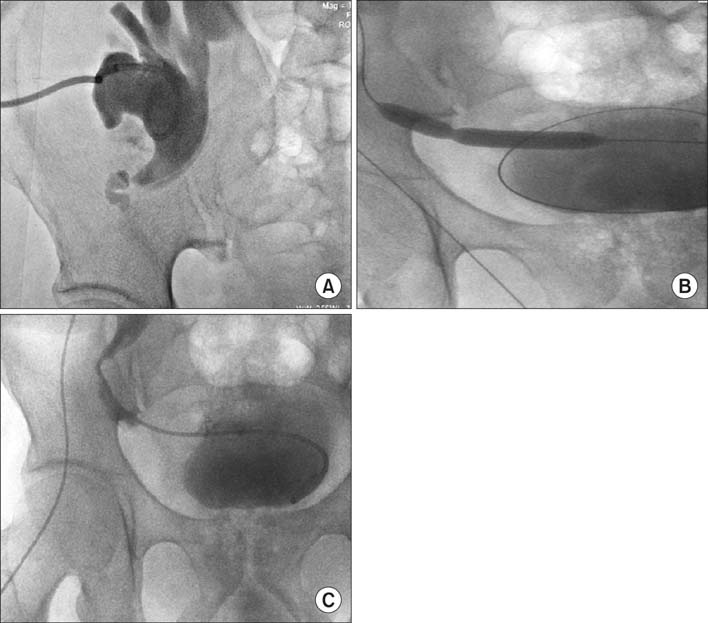
FIG. 2 Medical imaging of digital subtraction angiography: a 42-year-old patient with transplanted ureteric obstruction. (A) An external drainage catheter was inserted via the stiff guidewire with the distal portion coiled and located in the renal pelvis. (B) After external drainage for 46 hours, we successfully traversed the obstruction with a con ventional guidewire and exchanged it for a stiff guidewire. The balloon catheter was passed through the guidewire after ureteroplasty. (C) A double-J stent was inserted after balloon ureteroplasty.
Reference
-
1. Faenza A, Nardo B, Catena F, Scolari MP, d'Arcangelo GL, Buscaroli A, et al. Ureteral stenosis after kidney transplantation: a study on 869 consecutive transplants. Transpl Int. 1999; 12:334–340.2. Hobart MG, Streem SB, Gill IS. Renal transplant complications: minimally invasive management. Urol Clin North Am. 2000; 27:787–798.3. Kim BM, Park SI. Placement of double-J ureteric stent using the pull-through technique in patients with tight ureteric stenosis. Abdom Imaging. 2008; 33:237–240.4. Hausegger KA, Portugaller HR. Percutaneous nephrostomy and antegrade ureteral stenting: technique-indications-complications. Eur Radiol. 2006; 16:2016–2030.5. Atar E, Bachar GN, Bartal G, Mor E, Neyman H, Graif F, et al. Use of peripheral cutting balloon in the management of resistant benign ureteral and biliary strictures. J Vasc Interv Radiol. 2005; 16(2 Pt 1):241–245.6. Atar E, Bachar GN, Eitan M, Graif F, Neyman H, Belenky A. Peripheral cutting balloon in the management of resistant benign ureteral and biliary strictures: long-term results. Diagn Interv Radiol. 2007; 13:39–41.7. Keeling AN, Lee MJ. Crossing ureteric strictures: microcatheters to the rescue when conventional methods fail. Cardiovasc Intervent Radiol. 2007; 30:1234–1237.8. Govender P, Delaney H, Guiney M. Traversing tight ureteric strictures. Cardiovasc Intervent Radiol. 2009; 32:199–201.9. Kamiyama Y, Matsuura S, Kato M, Abe Y, Takyu S, Yoshikawa K, et al. Stent failure in the management of malignant extrinsic ureteral obstruction: risk factors. Int J Urol. 2011; 18:379–382.10. Karam G, Hetet JF, Maillet F, Rigaud J, Hourmant M, Soulillou JP, et al. Late ureteral stenosis following renal transplantation: risk factors and impact on patient and graft survival. Am J Transplant. 2006; 6:352–356.11. Giessing M. Transplant ureter stricture following renal transplantation: surgical options. Transplant Proc. 2011; 43:383–386.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Antegrade Ureteral Stenting in Ureteral Obstruction
- Effective Exchanging Method of Ureteral Stent in Patient with Severe Ureteral Stricture
- Effective Predicting Succes Factors of Retrograde Ureteral Stenting in Patients with Malignant Ureteral Obstruction
- A successful rendezvous endoscopic ultrasonography-guided gallbladder drainage in malignant cystic duct obstruction
- Clinical Observation on Cystoscopic Removal of Ureteral Stone using Woven Loop Stone Dislodger
