Placement of Endovascular Stent Graft in Acute Malperfusion Syndrome After Acute Type II Aortic Dissection
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Kyungpook National University Hospital, Daegu, Korea. straightroot@knu.ac.kr
- KMID: 2297897
- DOI: http://doi.org/10.4070/kcj.2012.42.9.638
Abstract
- Acute malperfusion syndrome is a serious complication of acute aortic dissection. A 76-year-old female patient was admitted with acute type B aortic dissection and developed renal malperfusion during medical therapy. We are reporting a clinically successful result from the thoracic endovascular aortic repair used for malperfusion syndrome that occurred by acute type B aortic dissection.
Keyword
Figure
-
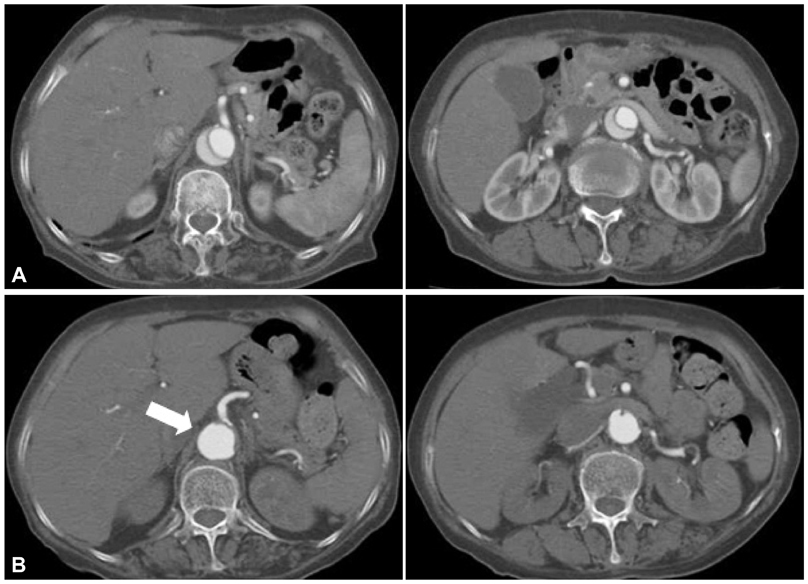
Fig. 1 Preoperative chest CT scans. A: the initial CT scan shows acute type B aortic dissection. B: follow-up chest CT scan shows that the size of true lumen of celiac artery and renal artery have been decreased significantly due to increasing false lumen pressure in descending aorta (the arrow indicates false lumen flow).
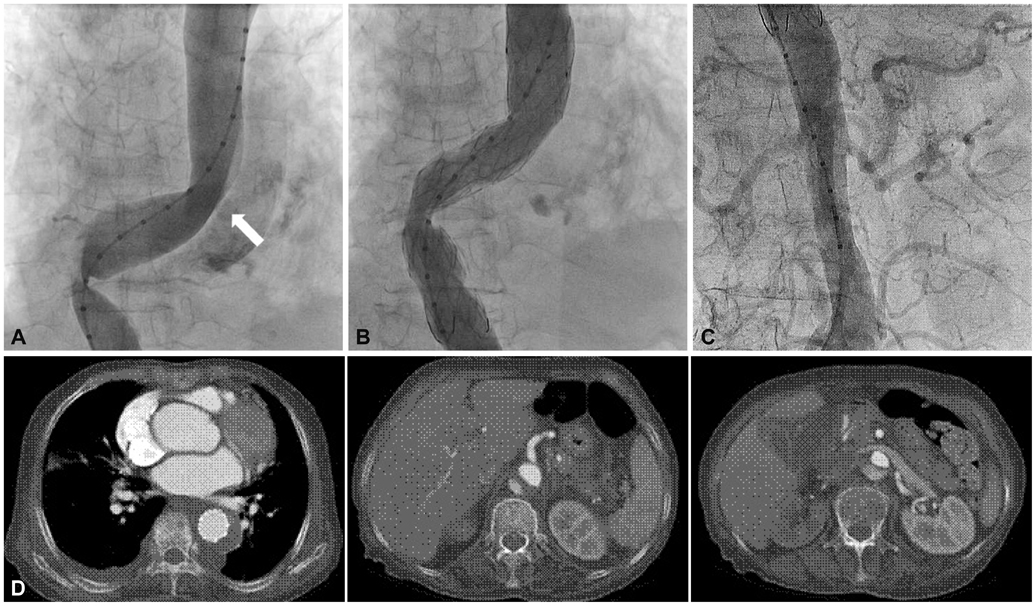
Fig. 2 Periperative aortograms and follow-up chest CT scans. A: the arrow indicates suspicious tearing site in aortogram. B: aortogram after thoracic endovascular aortic repair. Stent graft was positioned from distal thoracic aorta to just above celiac axis. C: restoration of blood flow in the abdominal branches after stent grafting. D: the postoperative CT scan shows that the size of true lumen in descending aorta have been increased and false lumen successfully have been obliterating.
Reference
-
1. Tsai TT, Fattori R, Trimarchi S, et al. Long-term survival in patients presenting with type B acute aortic dissection: insights from the International Registry of Acute Aortic Dissection. Circulation. 2006. 114:2226–2231.2. Lauterbach SR, Cambria RP, Brewster DC, et al. Contemporary management of aortic branch compromise resulting from acute aortic dissection. J Vasc Surg. 2001. 33:1185–1192.3. Williams DM, Lee DY, Hamilton BH, et al. The dissected aorta: part III. anatomy and radiologic diagnosis of branch-vessel compromise. Radiology. 1997. 203:37–44.4. Williams DM, Lee DY, Hamilton BH, et al. The dissected aorta: percutaneous treatment of ischemic complications--principles and results. J Vasc Interv Radiol. 1997. 8:605–625.5. Panneton JM, Teh SH, Cherry KJ Jr, et al. Aortic fenestration for acute or chronic aortic dissection: an uncommon but effective procedure. J Vasc Surg. 2000. 32:711–721.6. Suzuki T, Mehta RH, Ince H, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the International Registry of Aortic Dissection (IRAD). Circulation. 2003. 108:Suppl 1. II312–II317.7. Chen S, Yei F, Zhou L, et al. Endovascular stent-grafts treatment in acute aortic dissection (type B): clinical outcomes during early, late, or chronic phases. Catheter Cardiovasc Interv. 2006. 68:319–325.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complicated Acute Aortic Dissection with Malperfusion of the Left Common Iliac Artery Treated with Thoracic Endovascular Aortic Repair
- Thoracic Endovascular Repair for Complicated Type B Acute Aortic Dissection with Distal Malperfusion
- Retrograde Stanford type A aortic dissection after endovascular stent graft placement for type B dissection
- A Case of Complete Resolution of Aortic Dissection in the Descending Thoracic Aorta Treated with Endovascular Stent-Graft Implantation
- Mid-Term Results of Thoracic Endovascular Aortic Repair for Complicated Acute Type B Aortic Dissection at a Single Center
