Anatomical Factors Affecting Outcome of Outfracture of the Inferior Turbinate: Radiologic Analysis
- Affiliations
-
- 1Department of Otorhinolaryngology-Head & Neck Surgery, Dankook University College of Medicine, Cheonan, Korea. docjung@paran.com
- KMID: 2297552
- DOI: http://doi.org/10.18787/jr.2015.22.1.34
Abstract
- BACKGROUND AND OBJECTIVES
Outfracture of the inferior turbinate (IT) is a less invasive procedurethan all other reductive turbinate surgeries. The aim of this study is to investigate the anatomical factors of IT affecting outcomes of outfracture of the IT. MATERIALS AND METHOD: This study comprises 206 cases of 103 patients who underwent outfracture from 2006 to 2012. Patients weregrouped according to good outcome and poor outcome,based on postoperative endoscopic assessments after decongestion. Angle and length of IT, width of IT head, and the distance of the IT to the lateral nasal wall were compared at three different sections viacomputed tomography.
RESULTS
Significant differences in the length and angle of IT between the two groups were not found. The width of the IT head in the good outcome group was narrower than that in the poor outcome group. The distance of the IT to the lateral nasal wall was longer in the good outcome group, compared with that of the poor outcome group. These differences were especially prominent at the middle and posterior sections.
CONCLUSION
This study suggests that some anatomical factors, especially the width of the inferior meatus, could play a role in affecting the outcome of outfracture IT surgery.
Keyword
MeSH Terms
Figure
-
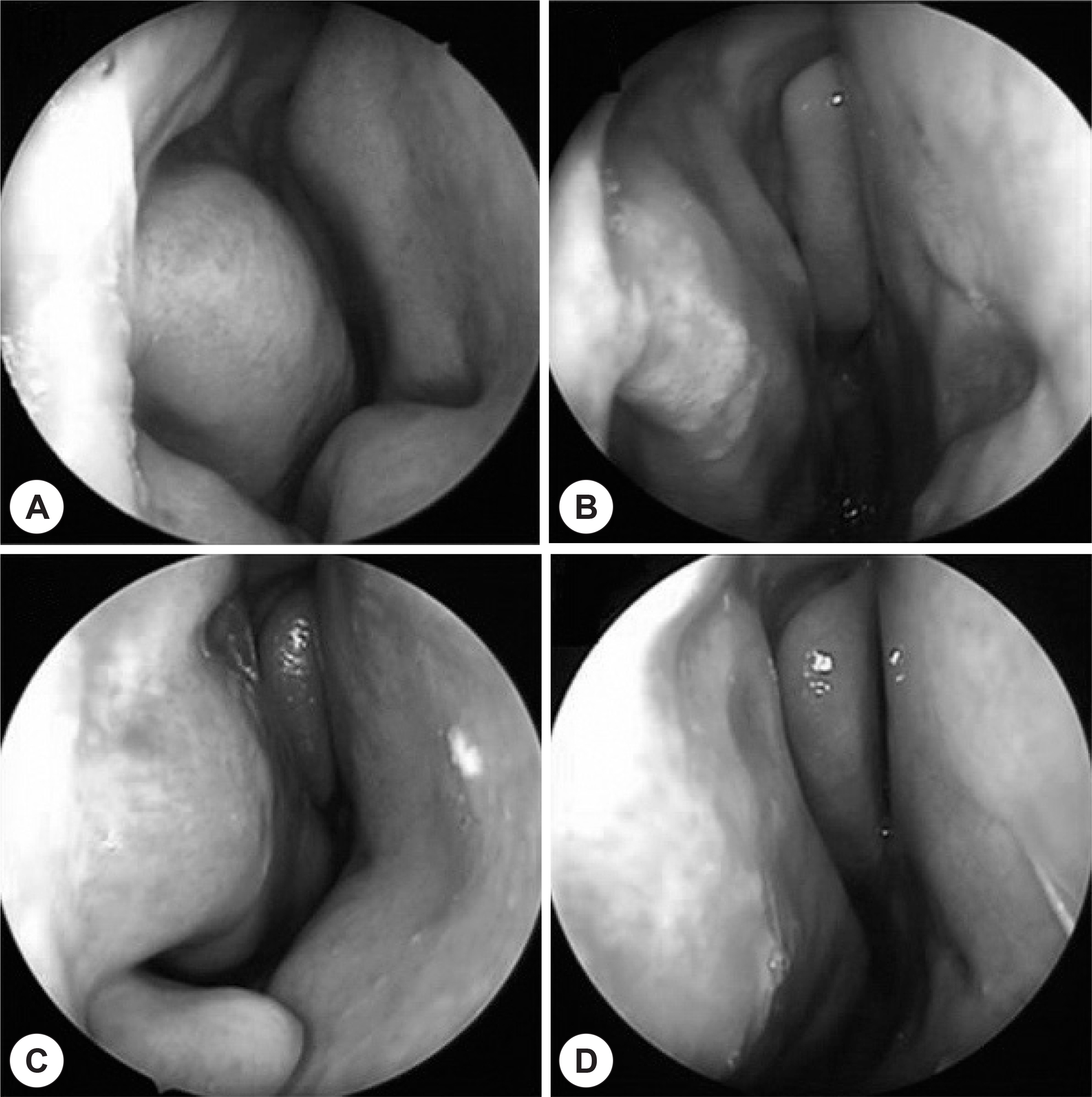
Fig. 1. Preoperative (A and C) and post-operative (B and D) endoscopic photographs of the good outcome patient (A and B) and poor outcome patient (C and D).

Fig. 2. A: The anterior section is the first scan, which could be seen entire inferior turbinate bone. B: The middle section is the scan at the level of the maxillary sinus ostium. C: The posterior section is the last scan, which could be seen entire the inferior turbinate bone.
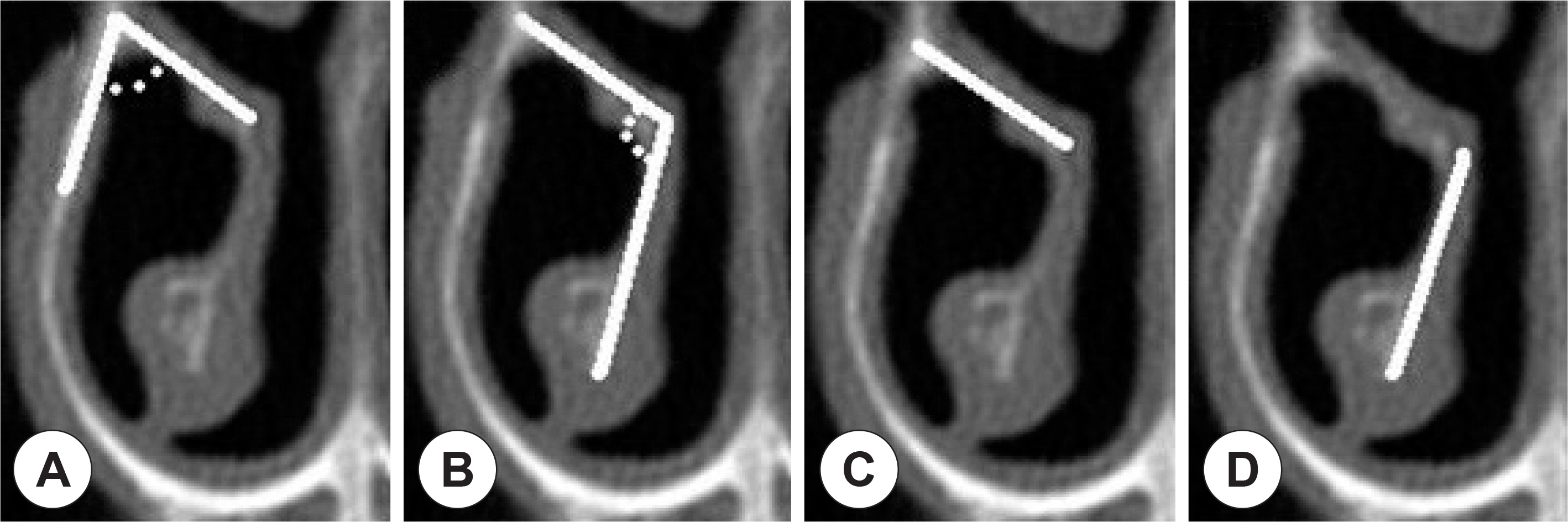
Fig. 3. Measurement of the angle, length of the inferior turbinate. A: 1st angle. B: 2nd angle. C: 1st length. D: 2nd length.
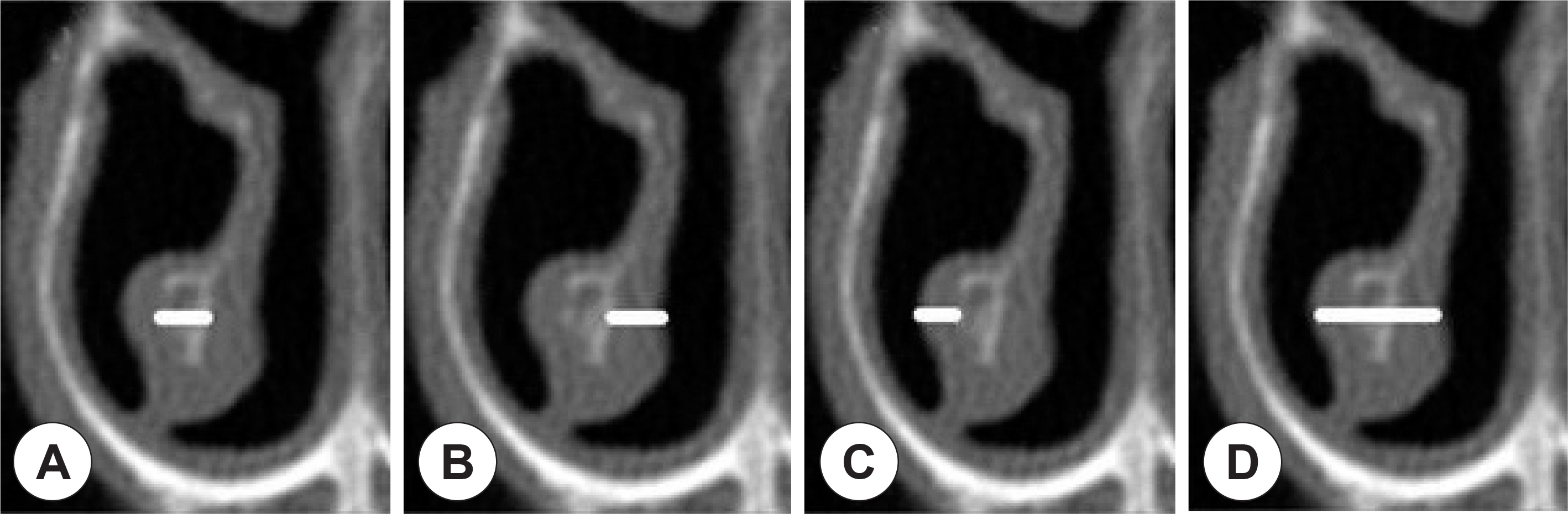
Fig. 4. The thickness of the inferior turbinate. A: Conchal bone. B: Medial mucosa. C: Lateral mucosa. D: Width of Head.
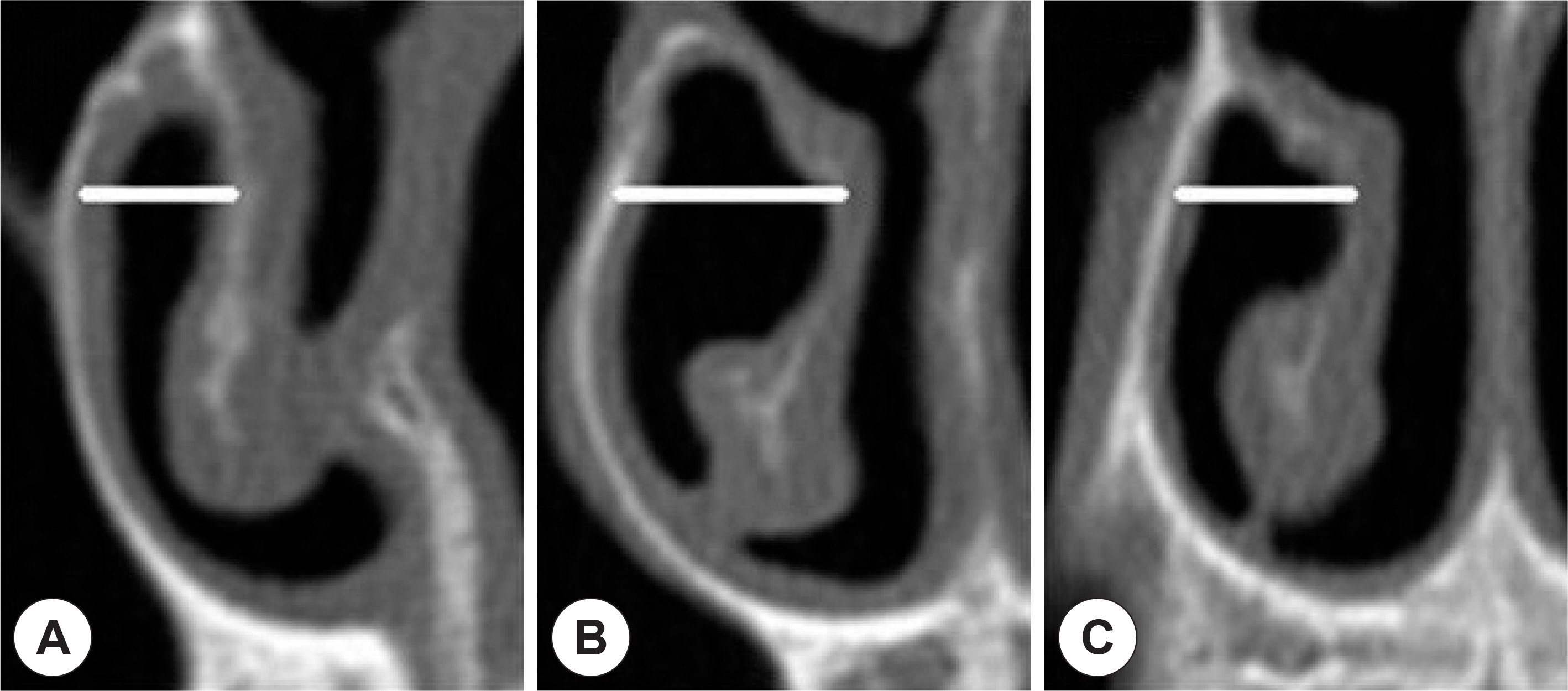
Fig. 5. Distances between the inferior turbinate bone and the lateral nasal wall. A: The anterior section. B: The middle section. C: The posterior section.
Reference
-
References
1). Bridger GP, Proctor DF. Maximum nasal inspiratory flow and nasal resistance. Ann Otol Rhinol Laryngol. 1970; 79(3):481–8.
Article2). McCombe AW, Cook J, Jones AS. A comparison of laser cautery and submucosal diathermy for rhinitis. Clin Otolaryngol Allied Sci. 1992; 17(4):297–9.
Article3). Jones AS, Wight RG, Kabil Y, Beckingham E. Predicting the outcome of submucosal diathermy to the inferior turbinates. Clin Otolaryngol Allied Sci. 1989; 14(1):41–4.
Article4). Richardson JR. Turbinate treatment in vasomotor rhinitis. Laryngoscope. 1948; 58(8):834–47.
Article5). Rohrich RJ, Krueger JK, Adams WP, Marple BF. Rationale for sub-mucous resection of hypertrophied inferior turbinates in rhinoplasty: an evolution. Plast Reconstr Surg. 2001; 108(2):536–46.
Article6). Gupta A, Mercurio E, Bielamowicz S. Endoscopic inferior turbinate reduction: an outcomes analysis. Laryngoscope. 2001; 111(11 Pt 1):1957–9.
Article7). Goode RL. Surgery of the turbinates. J Otolaryngol 1978;7(3):262–8.8). Buyuklu F, Cakmak O, Hizal E, Donmez FY. Outfracture of the Inferior Turbinate: A Computed Tomography Study. Plast Reconstr Surg. 2009; 123(6):1704–9.
Article9). Myung NS, Park BS, LEE HJ, Koo SK, Roh HJ. Analysis of Structural Changes of the Inferior Turbinate in Patients with Deviated Nasal Septum by Using Computed Tomography. Korean J Otorhi-nolaryngol-Head Neck Surg. 2008; 51(12):1104–8.10). Elahi MM, Frenkiel S, Fageeh N. Paraseptal stuructural changes and chronic sinus disease in relation to the deviated septum. J Otolaryngol. 1997; 26(4):236–40.11). Kim BH, Ryu JM, Cho YC, Lim DJ, Lee BY. Histopathology of the inferior turbinate showing compensatory hypertrophy in patients with deviated nasal septum. Korean J Otolaryngol. 2003; 46(3):230–3.12). McCombe AW, Cook J, Jones AS. A comparison of laser cautery and submucosal diathermy for rhinitis. Clin Otolaryngol Allied Sci. 1992; 17(4):297–9.
Article13). Min JY, Dhong HJ, Cho HJ, Chung SK, Kim HY. Evaluation of inferior turbinate outfracture outcomes using computed tomography. Rhinology. 2013; 51(3):275–9.
Article14). Chen YL, Tan CT, Huang HM. Longterm efficacy of microdebrider-assisted inferior turbinoplasty with lateralization for hypertrophic inferior turbinates in patients with perennial allergic rhinitis. Laryngoscope. 2008; 118(7):1270–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Inferior turbinate outfracture for successful nasotracheal intubation in a patient undergoing maxillofacial surgery: case report
- Structural Changes of Inferior Turbinate in Patients with Septal Deviation: Surgical Implication
- The First Case of a True Bifid Inferior Turbinate
- Application of inferior turbinate flap in cheiloplasty for wide cleft gaps
- Radiological Examinations of Inferior Turbinate in Patients with or without Deviated Nasal Septum by Using Computed Tomography
