Intramedullary Plate Fixation for the Comminuted Fracture of the Femoral Shaft: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea. taesado@naver.com
- KMID: 2297517
- DOI: http://doi.org/10.12671/jkfs.2007.20.4.345
Abstract
- A case of the comminuted fracture of the femoral shaft with osteoporosis is presented. The patient lacked sufficient bony stability and cortical bone-contact which allows union by conventional reconstruction method. Therefore, the authors performed a technique utilizing an intramedullary plate in combination with the standard lateral plate in order to obtain bony stabilization, early range of motion of the knee, and partial weight bearing ambulation and the technique is introduced.
Keyword
MeSH Terms
Figure
-

Fig. 1 Anteroposterior (AP) and lateral (Lat.) radiographs show the fracture of the left femoral shaft when patient visited ER: Winquist and Hansen classification type 1 (AO/ASIF - A1).

Fig. 2 AP radiographs show the postoperative state (B) of OR & IF with plating and bone grafts 7 months ago due to nonunion of the left femur subtrochanteric fracture (A) 14 years ago.

Fig. 3 AP and Lat. radiographs after 1st operation.

Fig. 4 AP and Lat. radiographs show that refracture between two plates which occurred 1 month after first operation: Winquist and Hansen classification type 3.
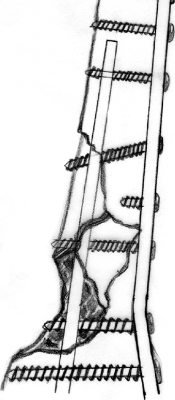
Fig. 5 The use of a broad dynamic compression plate (DCP, 12-hole) as a medial buttress, combined with a broad DCP (14-hole). The plate is fed into the intramedullary canal in a retrograde fashion and then, using the curved impactor. Two or three screws might thread the lateral cortex only and impact against the plate, pushing it medially (this picture does not illustrate). The other screws are inserted through the holes in both plates. To accomplish this, a 3.2 mm drill is used to drill the lateral cortex with the appropriate drill guide. A 1.6 mm Kirschner wire is then passed through the hole and is used to feel the hole of the medullary plate. When the direction is known, the drill is directed in the same path toward the medial cortex, which is penetrated. Insertion of these screws is frequently skewed so that the screws actually thread the hole in the plate as they pass into the medial cortex. In the drawing, the third screw from the top would have this effect [Illustration referred from Springer-Verlag, publisher3)].
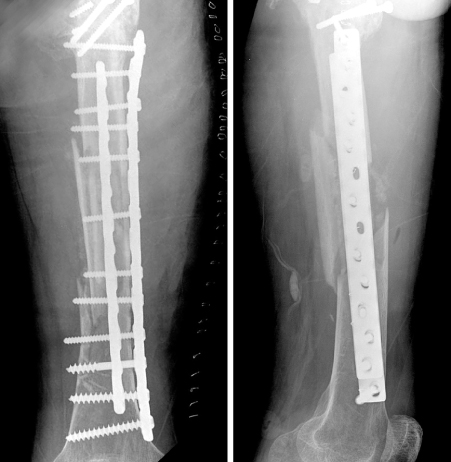
Fig. 6 Postoperative AP and Lat. radiographs: Intramedullary plate in combination with the lateral plate.

Fig. 7 AP and Lat. radiographs show complete union after 13 months.
Reference
-
1. Johnson EE. Custom titanium plating for failed nonunion or delayed internal fixation of femoral fractures. Clin Orthop Relat Res. 1988; 234:195–203.
Article2. Kim YM, Chung MS, Seong SC. Fracture. 1st ed. Seoul: Kwun-ja Inc;1977. p. 714–722.3. Mast J, Jakob R, Ganz R. Planning and Reduction Technique in Fracture Surgery. Berlin-heidelberg: Springer-Verlag;1989.4. Matelic TM, Monroe MT, Mast JW. The use of endosteal substitution in the treatment of recalcitrant nonunions of the femur: report of seven cases. J Orthop Trauma. 1996; 10:1–6.
Article5. Russell GV Jr, Pearsall AW. Intramedullary plate fixation of a distal humerus fracture: a case report. J Orthop Trauma. 2002; 16:353–356.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metal failure after compression plate fixation in femoral shaft fracture
- Operative Treatment of Femoral Shaft Fracture in Adult: Compression Plate Versus Intramedullary Nailing for Femoral Shaft Fracture
- Surgical Treatment of Ipsilateral Multi-Level Femoral Fracture Treated Using Antegrade Intramedullary Nail
- Comparative Study between Compression Plate with Screw Fixation and Interlocking Intramedullary Nailing of Tibial Shaft Fractures in Adult
- Comparative Clinical Study Between Plating and Intramedullary Nailing of Femoral Shaft Fractures in Adult
