Laparoscopic gonadectomy of streak gonads within the inguinal canals in a patient with XY partial gonadal dysgenesis
- Affiliations
-
- 1Department of Obstetrics and Gynecology, The Catholic University of Daegu School of Medicine, Daegu, Korea. drcys@cu.ac.kr
- 2Department of Pathology, The Catholic University of Daegu School of Medicine, Daegu, Korea.
- KMID: 2274130
- DOI: http://doi.org/10.5468/KJOG.2012.55.3.209
Abstract
- A 33-year-old phenotypic female presented with primary amenorrhea. The physical examination revealed no breast development, scanty axillary and pubic hair, normal female external genitalia, and a short blind vagina. The findings of magnetic resonance imaging, karyotyping, and hormonal examinations supported the diagnosis of XY partial gonadal dysgenesis. Laparoscopic surgery showed that spermatic cords, including the bilateral streak gonads and epididymes, were within the inguinal canals. After opening the spermatic cords and identifying the lower borders of the streak gonads, the spermatic cords were transected at the level of the vas deferens. A prophylactic herniorrhaphy using polyprophylene mesh was performed due to weakening of the internal inguinal ring. Pathologic evaluation of the gonads confirmed the diagnosis of partial gonadal dysgenesis without evidence of malignancy. A laparoscopic approach is feasible for treatment of XY gonadal dysgenesis, even if the streak gonads are present within the inguinal canal.
MeSH Terms
Figure
-
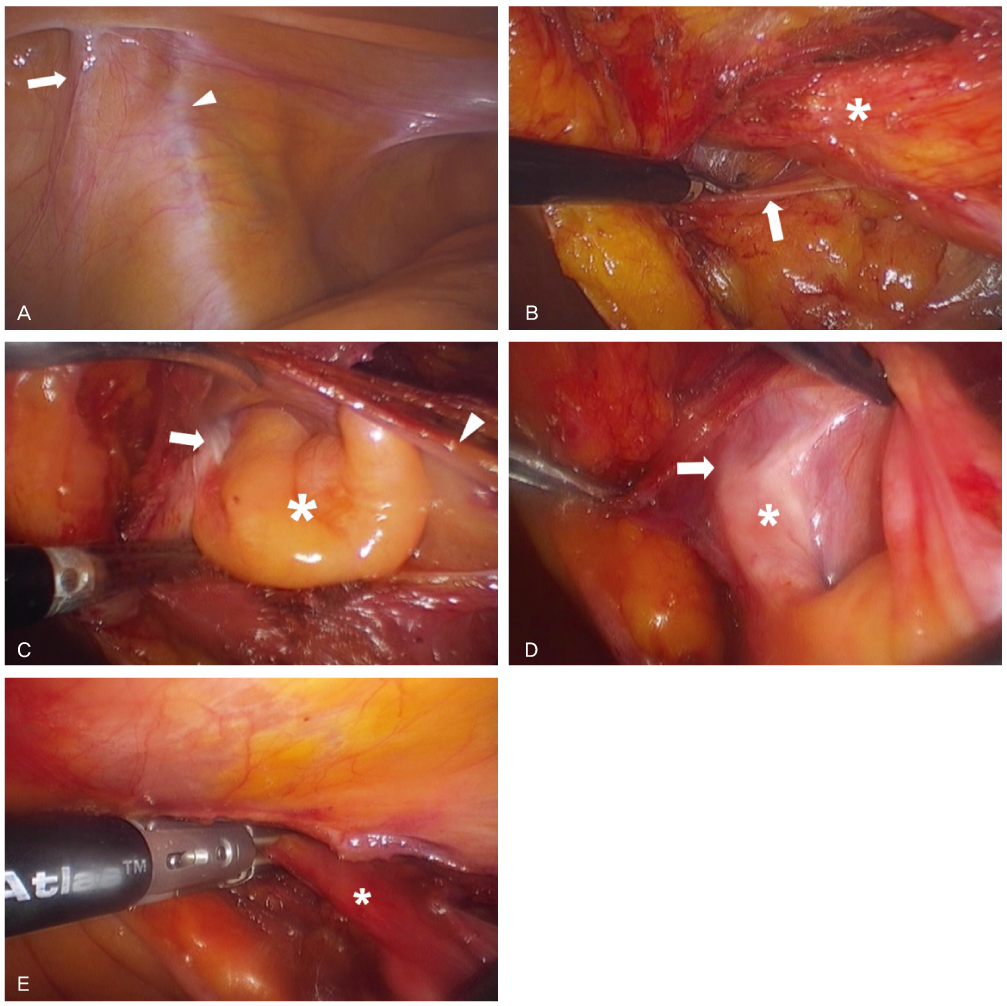
Fig. 1 Laparoscopic findings during surgery. (A) Left gonadal vessel (arrow) was identified lateral to the left external iliac artery (arrow head), and the distal ends of the gonadal vessel entered into the internal inguinal ring. (B) After peritoneal incision was made along the gonadal vessel, further dissection in the direction of the inguinal area revealed a spermatic cord (asterisk) and internal inguinal ring (arrow). (C) The spermatic cord (arrow head) was opened with monopolar scissors. A streak gonad (arrow), as a white band-like structure and epididymis (asterisk) was found in the spermatic cord. (D) Identifying the distal end (arrow) of the streak gonad (asterisk) (E) Vas deferens distal to the gonad was transected with LigaSure. Asterisk, spermatic cord.
Reference
-
1. Fechner PY, Marcantonio SM, Ogata T, Rosales TO, Smith KD, Goodfellow PN, et al. Report of a kindred with X-linked (or autosomal dominant sex-limited) 46,XY partial gonadal dysgenesis. J Clin Endocrinol Metab. 1993. 76:1248–1253.2. Verp MS, Simpson JL. Abnormal sexual differentiation and neoplasia. Cancer Genet Cytogenet. 1987. 25:191–218.3. Arici A, Kutteh WH, Chantilis SJ, Johns DA, Carr BR. Laparoscopic removal of gonads in women with abnormal karyotypes. J Reprod Med. 1993. 38:521–525.4. Droesch K, Droesch J, Chumas J, Bronson R. Laparoscopic gonadectomy for gonadal dysgenesis. Fertil Steril. 1990. 53:360–361.5. Yuen PM, Chan SS. Laparoscopy in a patient with XY gonadal dysgenesis. J Minim Invasive Gynecol. 2005. 12:194–195.6. Llorente J, Collins DL, Linarelli LG. Laparoscopic bilateral orchiectomy for testicular feminization syndrome. J Laparoendosc Surg. 1991. 1:351–353.7. Campo S, Garcea N. Laparoscopic gonadectomy in two patients with gonadal dysgenesis. J Am Assoc Gynecol Laparosc. 1998. 5:305–308.8. Kristiansen SB, Doody KJ. Laparoscopic removal of 46XY gonads located within the inguinal canals. Fertil Steril. 1992. 58:1076–1077.9. Dénes FT, Cocuzza MA, Schneider-Monteiro ED, Silva FA, Costa EM, Mendonca BB, et al. The laparoscopic management of intersex patients: the preferred approach. BJU Int. 2005. 95:863–867.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gonadoblastoma and dysgerminoma associated with 46,XY pure gonadal dysgenesis--a case report
- A case of Mixed Gonadal Dysgenesis Managed in Newborn Period
- A Case of Dysgerminoma Associated with 46, XY Pure Gonadal Dysgenesis
- A Case of Mos 45, X/46, XY Mixed Gonadal Dysgenesis
- A Case of 45 , X/46 , XY Mixed Gonadal Dysgenesis Associated with Azoospermia
