Ann Rehabil Med.
2012 Feb;36(1):33-38. 10.5535/arm.2012.36.1.33.
Reliability of Hip Migration Index in Children with Cerebral Palsy: The Classic and Modified Methods
- Affiliations
-
- 1Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul 120-752, Korea. pes1234@yuhs.ac
- KMID: 2266778
- DOI: http://doi.org/10.5535/arm.2012.36.1.33
Abstract
OBJECTIVE
To determine reliability and clinical use of two methods of migration index (MI) in CP patients with or without hip dysplasia. METHOD: The materials included radiographs of 200 hips of children with cerebral palsy. Conventional anteroposterior radiographs of the pelvis were taken with the child in the supine position with standardized methods. Two rehabilitation doctors measured the migration index using two methods. In the classic method, the lateral margin of the acetabular roof was used as a landmark and in the modified method the lateral margin of the sourcil was used as a landmark. Each rater measured the migration index at three separate times with a time interval of at least one week. Intraclass correlation (ICC) was used to test the inter- and intra-rater reliability.
RESULTS
MI shows excellent intra-rater reliability in both the classic and modified methods, but the inter-rater reliability was higher in the classic method than in the modified method. When categorized according to the sourcil classification, inter-rater reliability was higher in the normal sourcil type and lower in the dysplastic sourcil types.
CONCLUSION
Generally, the classic method showed higher reliability than the modified method, even though the reliability of the MI measurement was relatively high with both methods.
Keyword
Figure
-

Fig. 1 Sourcil (arrow) in the normal hip (A) and dysplastic hip (B).
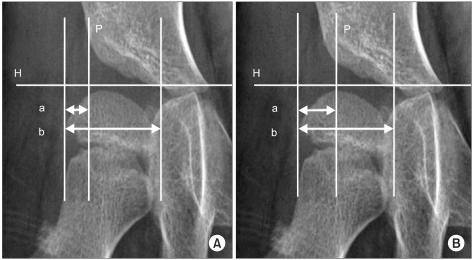
Fig. 2 Migration Index (MI) is measured with the classic method (A) and the modified method (B). H: Hilgenreiner's line, P: Perkin's line, MI=a/b×100 (%).
Reference
-
1. Gamble JG, Rinsky LA, Bleck EE. Established hip dislocation in children with cerebral palsy. Clin Orthop Relat Res. 1990; 253:90–99. PMID: 2180606.2. Laplaza FJ, Root L. Femoral anteversion and neck-shaft angles in hip instability in cerebral palsy. J Pediatr Orthop. 1994; 14:719–723. PMID: 7814583.
Article3. Hagglund G, Andersson S, Duppe H, Lauge-Pedersen H, Nordmark E, Westbom L. Prevention of dislocation of the hip in children with cerebral palsy. The first ten years of a population-based prevention programme. J Bone joint Surg Br. 2005; 87:95–101. PMID: 15686244.4. Reimers J. The stability of the hip in children. A radiological study of the results of muscle surgery in cerebral palsy. Acta Orthop Scand Suppl. 1980; 184:1–100. PMID: 6930145.
Article5. Parrott J, Boyd RN, Dobson F, Lancaster A, Love S, Oates J, Wolfe R, Nattrass GR, Graham HK. Hip displacement in spastic cerebral palsy: repeatability of radiologic measurement. J Pediatr Orthop. 2002; 22:660–667. PMID: 12198471.
Article6. Pountney T, Mandy A, Gard P. Repeatability and limits of agreement in measurement of hip migration percentage in children with bilateral cerebral palsy. Physiotherapy. 2003; 89:276–281.
Article7. Faraj S, Atherton WG, Stott NS. Inter- and intra-measurer error in the measurement of Reimers' hip migration percentage. J Bone Joint Surg Br. 2004; 86:434–437. PMID: 15125134.
Article8. Agus H, Bicimoqlu A, Omeroglu H, Tumer Y. How should the acetabular angle of Sharp be measured on a pelvic radiograph? J Pediatr Orthop. 2002; 22:228–231. PMID: 11856937.
Article9. Armand M, Lepisto J, Tallroth K, Elias J, Chao E. Outcome of periacetabular osteotomy: joint contact pressure calculation using standing AP radiographs, 12 patients followed for average 2 years. Acta Orthop. 2005; 76:303–313. PMID: 16156455.10. Broughton NS, Brougjman DI, Cole WG, Menelaus MB. Reliability of radiological measurement in the assessment of the child's hip. J Bone Joint Surg Br. 1989; 71:6–8. PMID: 2915007.11. Kim HT, Kim JI, Yoo CI. Diagnosing childhood acetabular dysplasia using the lateral margin of the sourcil. J Pediatr Orthop. 2000; 20:709–717. PMID: 11097241.
Article12. Lonstein JE, Beck K. Hip dislocation and subluxation in cerebral palsy. J Pediatr Orthop. 1986; 6:521–526. PMID: 3760161.
Article13. Ogata S, Moriya H, Tsuchiya K, Akita T, Kamegaya N, Someya M. Acetabular cover in congenital dislocation of the hip. J Bone Joint Surg Br. 1990; 72:190–196. PMID: 2312554.
Article14. Scrutton D. The early management of hips in cerebral palsy. Dev Med Child Neurol. 1989; 31:108–116. PMID: 2646162.
Article15. Shea KG, Coleman SS, Carroll K, Stevens P, Van Boerum DH. Pemberton pericapsular osteotomy to treat a dysplastic hip in cerebral palsy. J Bone Joint Surg Am. 1997; 79:1342–1351. PMID: 9314396.
Article16. Cottalorda J, Gautheron V, Metton G, Charmet E, Maatougui K, Chavrier Y. Predicting the outcome of adductor tenotomy. Int Orthop. 1998; 22:374–379. PMID: 10093805.
Article17. Heim RC, Park TS, Vogler GP, Kaufman BA, Noetzel MJ, Ortman MR. Changes in hip migration after selective dorsal rhizotomy for spastic quadriplegia in cerebral palsy. J Neurosurg. 1995; 82:567–571. PMID: 7897515.
Article18. Onimus M, Allamel G, Manzone P, Laurain JM. Prevention of hip dislocation in cerebral palsy by early psoas and adductors tenotomies. J Pediatr Orthop. 1991; 11:432–435. PMID: 1860938.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early Subluxation of Hip in Children with Cerebral Palsy
- Hip Migration after Selective Posterior Rhizotomy in Cerebral Palsy
- Hip Subluxation according to Neuromotor Type and Motor Quotient in Patients with Cerebral Palsy
- The Effect of Obturator Nerve Block on Hip Lateralization in Low Functioning Children with Spastic Cerebral Palsy
- Early Results of One-Stage Correction for Hip Instability in Cerebral Palsy
