Sciatic Nerve Injury Caused by a Stretching Exercise in a Trained Dancer
- Affiliations
-
- 1Department of Rehabilitation Medicine, Michuhol Rehabilitation Center, Incheon, Korea. oklim0928@yahoo.co.kr
- 2Department of Rehabilitation Medicine, Gachon University of Medicine and Science, Incheon, Korea.
- 3Department of Radiology, Incheon Imaging Diagnostic Center, Incheon, Korea.
- KMID: 2266569
- DOI: http://doi.org/10.5535/arm.2013.37.6.886
Abstract
- Sciatic nerve injury after stretching exercise is uncommon. We report a case of an 18-year-old female trained dancer who developed sciatic neuropathy primarily involving the tibial division after routine stretching exercise. The patient presented with dysesthesia and weakness of the right foot during dorsiflexion and plantarflexion. The mechanism of sciatic nerve injury could be thought as hyperstretching alone, not caused by both hyperstretching and compression. Electrodiagnostic tests and magnetic resonance imaging revealed evidence of the right sciatic neuropathy from the gluteal fold to the distal tibial area, and partial tear of the left hamstring origin and fluid collection between the left hamstring and ischium without left sciatic nerve injury. Recovery of motor weakness was obtained by continuous rehabilitation therapy and some evidence of axonal regeneration was obtained by follow-up electrodiagnostic testing performed at 3, 5, and 12 months after injury.
MeSH Terms
Figure
-
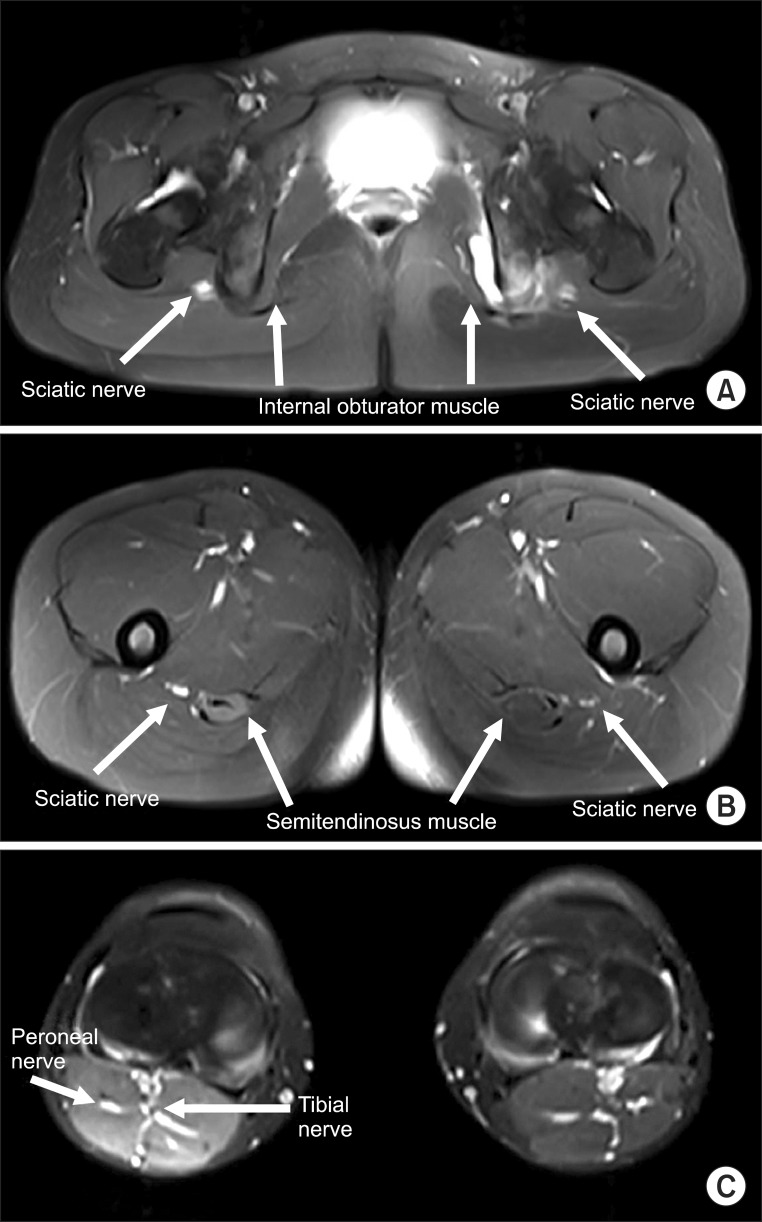
Fig. 1 FS T2 WI-axial scans. (A) FS T2 WI-axial scan at the level of the ischial spine shows stretching injury with abnormal high signal intensity in the right sciatic nerve, and left partial tear with high signal hemorrhagic fluid accumulation on left internal obturator muscle at insertion and the hamstring muscle origin. No definite mass lesion compressing or contacting the right sciatic nerve was found. Left sciatic nerve is contacting the above lesions, but not enlarged or edematous. (B) FS T2 WI-axial scan at the level of the mid femoral shaft shows continuous higher signal intensity through the right sciatic nerve, relative to left normal sciatic nerve with intermediate signal intensity. (C) FS T2 WI-axial scan at the level of the knee shows multiple denervation change with diffusely high signal intensity at the right distal biceps femoris muscle, right semitendinosus muscle, and both medial and lateral gastrocnemius muscles. FS, fat saturation; T2 WI, T2-weighted image.
Reference
-
1. Hyun JK, Lee SJ, Yoo DS, Park HG, Kwon BS. The electrodiagnostic findings of sciatic nerve injury according to the locations and etiologies. J Korean Acad Rehabil Med. 2004; 28:54–58.2. Krivickas LS, Wilbourn AJ. Sports and peripheral nerve injuries: report of 190 injuries evaluated in a single electromyography laboratory. Muscle Nerve. 1998; 21:1092–1094. PMID: 9655133.
Article3. Kouyoumdjian JA. Peripheral nerve injuries: a retrospective survey of 456 cases. Muscle Nerve. 2006; 34:785–788. PMID: 16881066.
Article4. Kwon IS, Bang HJ. A case report of bilateral sciatic neuropathy after sleeping with cross-legged position. J Korean Assoc EMG Electrodiagn Med. 2007; 9:189–192.5. Walker M, Meekins G, Hu SC. Yoga neuropathy: a snoozer. Neurologist. 2005; 11:176–178. PMID: 15860140.6. Dumitru D, Amato AA, Zwarts MJ. Peripheral nervous system's reaction to injury. Electrodiagnostic medicine. 2nd ed. Philadelphia: Hanley & Belfus;2002. p. 115–158.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Femoral and Sciatic Nerve Palsy Associated with Acetabular Fracture and Dislocation: A Case Report
- Opposite Sciatic Nerve Injury after Fixation of Femur Shaft Fracture: Two case reports
- Effect of Exercise Training on Histochemical Muscle Recovery after Sciatic Nerve Crush in Rat
- Histochemical Findings of Soleus in Relation to the Severity of Injury and Duration of Exercise in Sciatic Nerve Injured Rats
- Sciatic Nerve Compression due to Ganglion
