Diffusion Tensor Tractography in Two Cases of Kernohan-Woltman Notch Phenomenon
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea. rmpyun@korea.ac.kr
- KMID: 2266568
- DOI: http://doi.org/10.5535/arm.2013.37.6.879
Abstract
- Kernohan-Woltman notch phenomenon (KWP) is an ipsilateral motor weakness due to compression of the contralateral cerebral peduncle. We report two cases of KWP following traumatic brain injury. In case 1, ipsilateral hemiplegia was noted after right subdural hemorrhage. Although magnetic resonance imaging showed no abnormal signal changes on cerebral peduncle, diffusion tensor tractography (DTT) revealed interruption of corticospinal tract (CST) at lower level of the midbrain level. In case 2, there was abnormal signal change of the right cerebral peduncle contralateral to the primary lesion and we could not reconstruct right CST. Case 1 showed unsatisfactory motor recovery even after 15 months, and follow-up DTT showed no change. In case 2, follow-up DTT was not performed, but her ipsilateral hemiparesis had almost disappeared during the 15 months. DTT would be useful in detecting ipsilateral hemiparesis due to KWP and the clinical course may differ according to the lesion characteristics.
MeSH Terms
Figure
-
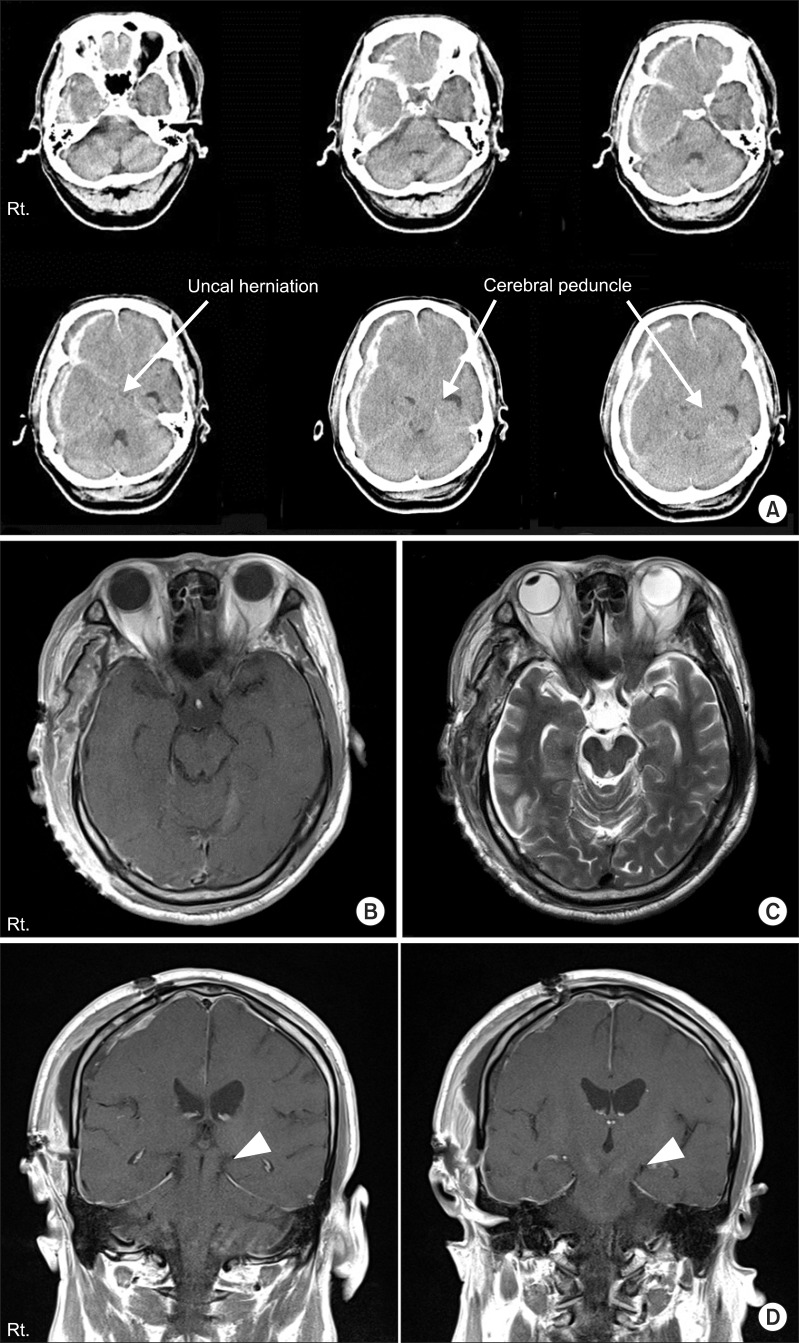
Fig. 1 (A) Brain computed tomography at the onset of injury in case 1. The images show massive subdural hemorrhage on the right frontotemporal lobe with uncal herniation to the left causing compression of the cerebral peduncle against the tentorial egde (arrows). (B) The T1- and (C) T2-weighted axial magnetic resonance (MR) images 5 days after injury. (D) T1-weighted coronal MR images 5 days after injury. The uncal herniation improved after surgery but the images showed mild shifting of cerebral peduncle to the left tentorial edge (arrow heads). There were no abnormal signal changes on MR images.
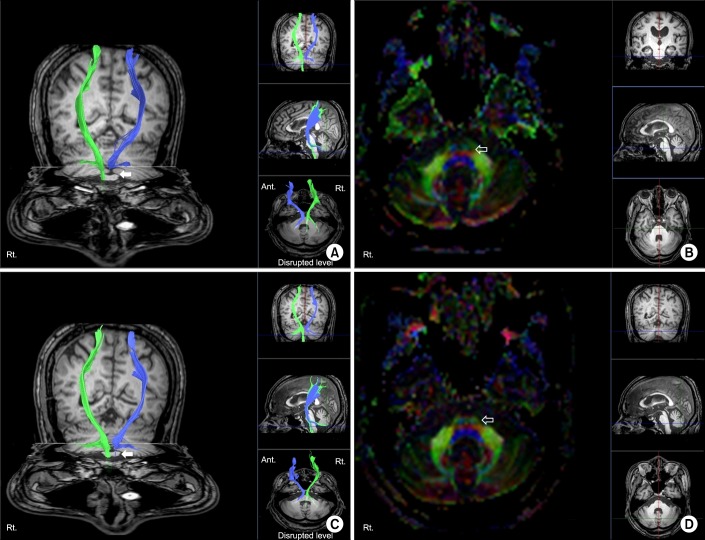
Fig. 2 (A) Diffusion tensor image with tractography for the corticospinal tract and (B) axial image of the fractional anisotropy (FA) color map 4 weeks after the onset of injury. (C) Follow-up tractography and (D) axial image of FA color map 9 months after the onset of injury (left hemisphere, blue; right hemisphere, green). Disruptions of corticospinal tract around the left pons were noted in initial and follow-up images (arrows). FA color map showed disrupted blue fibers in the left anterior pons compared with the right side (open arrows).
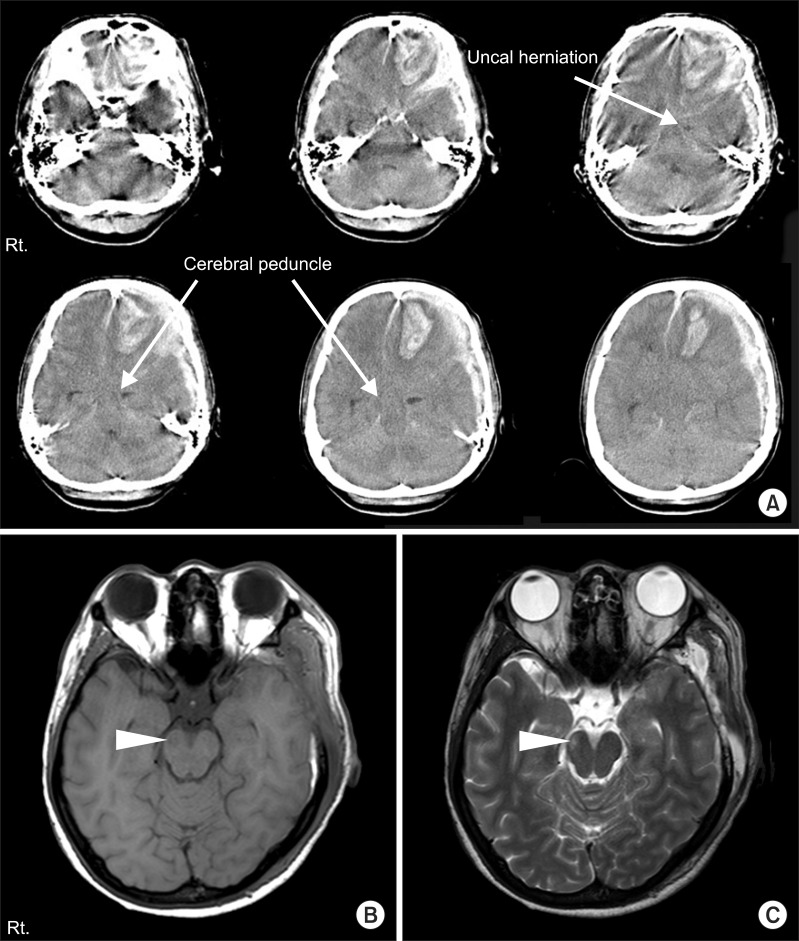
Fig. 3 (A) Brain computed tomography at the onset of injury in case 2. The images show a large amount of left frontotemporal subdural hemorrhage, frontal intracranial hemorrhage, and contralateral shift of midline and transtentorial herniation (arrows). (B) The T1- and (C) T2-weighted axial magnetic resoance images 10 days after injury. Low intensity signal change in the right crus cerebri on T1-weighted image, and high signal intensity change on T2-weighted image (arrow heads).
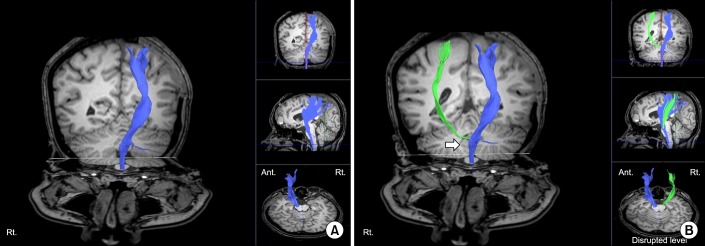
Fig. 4 (A) Diffusion tensor image with tractography (DTT) for the corticospinal tract (CST) 8 weeks after the onset of injury in case 2 (left hemisphere, blue). Although tentorial herniation caused brain stem damage in Kernohan-Woltman notch phenomenon, right CST tract was also not visualized from cerebral cortex to posterior limb of internal capsule (PLIC) after reconstruction, which was not the case in DTT image of case 1. (B) CST was reconstructed after using different region of interest (ROI) method. One ROI was placed on the CST portion of the anterior mid pons and the other was placed on the CST portion of PLIC (left hemisphere, blue; right hemisphere, green). Disruption of CST around midbrain level was noted (arrow).
Reference
-
1. Zafonte RD, Lee CY. Kernohan-Woltman notch phenomenon: an unusual cause of ipsilateral motor deficit. Arch Phys Med Rehabil. 1997; 78:543–545. PMID: 9161379.
Article2. Kernohan JW, Woltman HW. Incisura of the crus due to contralateral brain tumor. Arch Neurol Psychiatry. 1929; 21:274–287.
Article3. Yoo WK, Kim DS, Kwon YH, Jang SH. Kernohan's notch phenomenon demonstrated by diffusion tensor imaging and transcranial magnetic stimulation. J Neurol Neurosurg Psychiatry. 2008; 79:1295–1297. PMID: 18940992.
Article4. Cho HK, Hong JH, Kim SH, Kim OL, Ahn SH, Jang SH. Clinical usefulness of diffusion tensor imaging in patients with transtentorial herniation following traumatic brain injury. Brain Inj. 2011; 25:1005–1009. PMID: 21812586.
Article5. Gentry LR, Godersky JC, Thompson B. MR imaging of head trauma: review of the distribution and radiopathologic features of traumatic lesions. AJR Am J Roentgenol. 1988; 150:663–672. PMID: 3257624.
Article6. Gentry LR, Godersky JC, Thompson BH. Traumatic brain stem injury: MR imaging. Radiology. 1989; 171:177–187. PMID: 2928523.
Article7. Kole MK, Hysell SE. MRI correlate of Kernohan's notch. Neurology. 2000; 55:1751. PMID: 11113240.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Motor Symptoms in Brain Stem Lesion
- Reversible Psychosis Caused by Disconnection of the Limbic System: Clinical Reasoning Using Diffusion Tensor Tractography
- Diffusion Tensor Imaging: Exploring the Motor Networks and Clinical Applications
- Usefulness of Diffusion Tensor Imaging in Unexplained Ipsilateral Hemiplegia
- Preoperative Identification of Facial Nerve in Vestibular Schwannomas Surgery Using Diffusion Tensor Tractography
