Threshold of Clinical Severity of Cervical Dystonia for Positive 18F-FDG PET/CT
- Affiliations
-
- 1The Clinic for Torticollis, Department of Physical Medicine and Rehabilitation, Ajou University School of Medicine, Suwon, Korea. syyim@ajou.ac.kr
- 2Department of Nuclear Medicine and Molecular Imaging, Ajou University School of Medicine, Suwon, Korea.
- 3Department of Neurosurgery, Ajou University School of Medicine, Suwon, Korea.
- KMID: 2266556
- DOI: http://doi.org/10.5535/arm.2013.37.6.777
Abstract
OBJECTIVE
To examine whether the clinical severity of cervical dystonia (CD) significantly correlates with 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) findings as well as to determine the threshold of the clinical severity of CD for positive 18F-FDG PET/CT study findings.
METHODS
Forty-seven subjects with torticollis as one of the symptoms of CD were included. The clinical severity of CD was evaluated with the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) at the time of 18F-FDG PET/CT. The correlation between the clinical severity of CD and the highest SUVmax was examined. The threshold of the clinical severity of CD necessary for positive 18F-FDG PET/CT findings was determined using receiver operating characteristics curve analysis.
RESULTS
Thirty-three of the 47 subjects (70.21%) showed positive 18F-FDG PET/CT findings. The ipsilateral splenius capitis/cervicis, oblique capitis inferior, and longus colli/capitis were the rotators most frequently involved. The highest SUVmax of 18F-FDG PET/CT was significant correlated with the TWSTRS. Subjects with a total TWSTRS exceeding 39 showed positive 18F-FDG PET/CT findings, with those having a total TWSTRS < or =22 showing negative 18F-FDG PET/CT results. The cutoff value of the total TWSTRS for positive 18F-FDG PET/CT findings was set at 27.5 with 90.9% sensitivity and 64.3% specificity.
CONCLUSION
A significant correlation was evident between the clinical severity of CD and 18F-FDG PET/CT findings, providing a threshold of the clinical severity of CD for acquisition of positive 18F-FDG PET/CT findings.
MeSH Terms
Figure
-

Fig. 1 (A-C) Correlation between TWSTRS and the highest SUVmax of 18F-fluorodeoxyglucose positron emission tomography/computed tomography. The SUVmax showed significant correlation with (A) the total TWSTRS, (B) severity subscale scores, and (C) disability subscale scores of TWSTRS (p<0.001). (D) There was no correlation between the scores of pain subscale and the SUVmax (p=0.582). The highest value among SUVmaxes of 10 rotators in each subject was defined as the highest SUVmax. SUVmax, maximum standardized uptake value; TWSTRS, Toronto Western Spasmodic Torticollis Rating Scale.
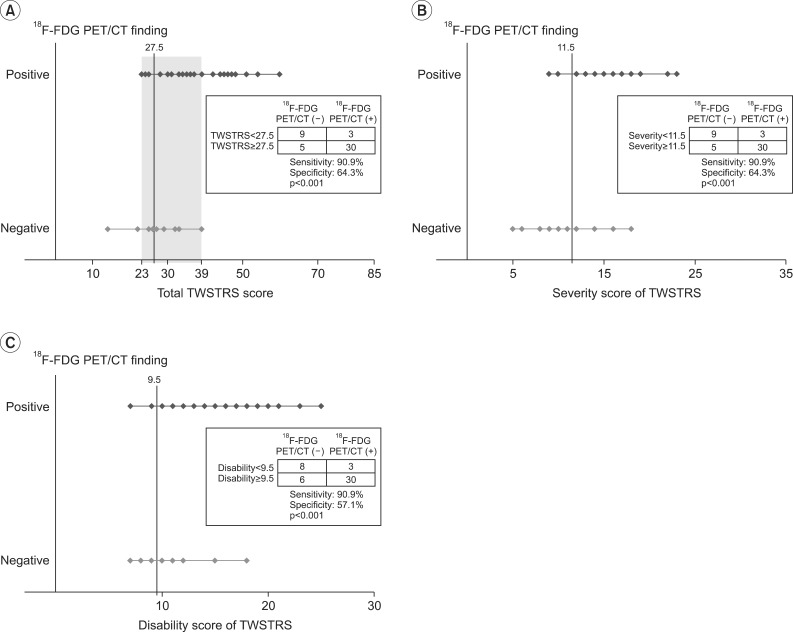
Fig. 2 Optimal cutoff value of TWSTRS for 18F-FDG PET/CT positive finding selected by receiver operating characteristics curve analysis. (A) The cutoff value of total score of TWSTRS was 27.5. The lowest total score of TWSTRS for the positive 18F-FDG PET/CT findings was 23. All subjects with a total TWSTRS of more than 39 showed positive 18F-FDG PET/CT findings. (B) The cutoff value of severity score of TWSTRS was 11.5. (C) The cutoff value of disability score of TWSTRS was 9.5. TWSTRS, Toronto Western Spasmodic Torticollis Rating Scale; 18F-FDG PET/CT, 18F-fluorodeoxyglucose positron emission tomography/computed tomography.
Reference
-
1. Jankovic J, Tolosa E. Parkinson's disease and movement disorders. 5th ed. Philadelphia: Lippincott Williams & Wilkins;2007.2. Jankovic J, Tsui J, Bergeron C. Prevalence of cervical dystonia and spasmodic torticollis in the United States general population. Parkinsonism Relat Disord. 2007; 13:411–416. PMID: 17442609.
Article3. Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group. A prevalence study of primary dystonia in eight European countries. J Neurol. 2000; 247:787–792. PMID: 11127535.4. Camargo CH, Teive HA, Becker N, Baran MH, Scola RH, Werneck LC. Cervical dystonia: clinical and therapeutic features in 85 patients. Arq Neuropsiquiatr. 2008; 66:15–21. PMID: 18392407.
Article5. Albanese A, Barnes MP, Bhatia KP, Fernandez-Alvarez E, Filippini G, Gasser T, et al. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force. Eur J Neurol. 2006; 13:433–444. PMID: 16722965.
Article6. Brans JW, de Boer IP, Aramideh M, Ongerboer de Visser BW, Speelman JD. Botulinum toxin in cervical dystonia: low dosage with electromyographic guidance. J Neurol. 1995; 242:529–534. PMID: 8530982.
Article7. Comella CL, Buchman AS, Tanner CM, Brown-Toms NC, Goetz CG. Botulinum toxin injection for spasmodic torticollis: increased magnitude of benefit with electromyographic assistance. Neurology. 1992; 42:878–882. PMID: 1565246.
Article8. Anderson TJ, Rivest J, Stell R, Steiger MJ, Cohen H, Thompson PD, et al. Botulinum toxin treatment of spasmodic torticollis. J R Soc Med. 1992; 85:524–529. PMID: 1433117.9. Truong D, Duane DD, Jankovic J, Singer C, Seeberger LC, Comella CL, et al. Efficacy and safety of botulinum type A toxin (Dysport) in cervical dystonia: results of the first US randomized, double-blind, placebo-controlled study. Mov Disord. 2005; 20:783–791. PMID: 15736159.
Article10. Jankovic J. Treatment of cervical dystonia with botulinum toxin. Mov Disord. 2004; 19(Suppl 8):S109–S115. PMID: 15027062.
Article11. Brans JW, Aramideh M, Koelman JH, Lindeboom R, Speelman JD, Ongerboer de Visser BW. Electromyography in cervical dystonia: changes after botulinum and trihexyphenidyl. Neurology. 1998; 51:815–819. PMID: 9748032.12. Sung DH, Choi JY, Kim DH, Kim ES, Son YI, Cho YS, et al. Localization of dystonic muscles with 18F-FDG PET/CT in idiopathic cervical dystonia. J Nucl Med. 2007; 48:1790–1795. PMID: 17942812.
Article13. Lee HB, An YS, Lee HY, Hwang JH, Lee HJ, Jeong KY, et al. Usefulness of (18)f-fluorodeoxyglucose positron emission tomography/computed tomography in management of cervical dystonia. Ann Rehabil Med. 2012; 36:745–755. PMID: 23342305.14. Yim SY, Lee IY, Park MC, Kim JH. Differential diagnosis and management of abnormal posture of the head and neck. J Korean Med Assoc. 2009; 52:705–718.
Article15. Consky ES, Lang AE. Clinical assessments of patients with cervical dystonia. Neurol Dis Ther. 1994; 25:211.16. Salvia P, Champagne O, Feipel V, Rooze M, de Beyl DZ. Clinical and goniometric evaluation of patients with spasmodic torticollis. Clin Biomech (Bristol, Avon). 2006; 21:323–329.
Article17. An YS, Sheen SS, Oh YJ, Hwang SC, Yoon JK. Nonionic intravenous contrast agent does not cause clinically significant artifacts to 18F-FDG PET/CT in patients with lung cancer. Ann Nucl Med. 2007; 21:585–592. PMID: 18092135.
Article18. An YS, Sun JS, Park KJ, Hwang SC, Park KJ, Sheen SS, et al. Diagnostic performance of (18)F-FDG PET/CT for lymph node staging in patients with operable non-small-cell lung cancer and inflammatory lung disease. Lung. 2008; 186:327–336. PMID: 18670805.
Article19. Lee IH, Yoon YC, Sung DH, Kwon JW, Jung JY. Initial experience with imaging-guided intramuscular botulinum toxin injection in patients with idiopathic cervical dystonia. AJR Am J Roentgenol. 2009; 192:996–1001. PMID: 19304706.
Article20. Jankovic J, Leder S, Warner D, Schwartz K. Cervical dystonia: clinical findings and associated movement disorders. Neurology. 1991; 41:1088–1091. PMID: 2067638.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between 18F-FDG PET/CT and EMG Mapping for Identifying Dystonic Superficial Muscles in Primary Cervical Dystonia: Preliminary Results
- Verification of the Dystonic Muscles Using 18F-Fluorodeoxyglucose Positron Emission Tomography in a Patient with Cervical Dystonia: A case report
- Use of 18F-FDG PET/CT in Second Primary Cancer
- 18F-FDG PET/CT and Sonographic Findings of Thyroid Incidentalomas
- Esophageal Leiomyoma with intense FDG uptake on 18F-FDG PET/CT
