Clin Orthop Surg.
2015 Sep;7(3):330-336. 10.4055/cios.2015.7.3.330.
Results of Corrective Osteotomy and Treatment Strategy for Ankylosing Spondylitis with Kyphotic Deformity
- Affiliations
-
- 1Department of Orthopaedic Surgery, Spine Center, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- 2Department of Orthopedic Surgery, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. 97111033@hanmail.net
- KMID: 2234087
- DOI: http://doi.org/10.4055/cios.2015.7.3.330
Abstract
- BACKGROUND
To report the radiological and clinical results after corrective osteotomy in ankylosing spondylitis patients. Furthermore, this study intended to classify the types of deformity and to suggest appropriate surgical treatment options.
METHODS
We retrospectively analyzed ankylosing spondylitis patients who underwent corrective osteotomy between 1996 and 2009. The radiographic assessments included the sagittal vertical axis (SVA), spinopelvic alignment parameters, correction angle, correction loss, type of deformity related to the location of the apex, and the craniocervical range of motion (CCROM). The clinical outcomes were assessed by the Oswestry Disability Index (ODI) scores.
RESULTS
A total of 292 corrective osteotomies were performed in 248 patients with a mean follow-up of 40.1 months (range, 24 to 78 months). There were 183 cases of single pedicle subtraction osteotomy (PSO), 19 cases of multiple Smith-Petersen osteotomy (SPO), 17 cases of PSO + SPO, 14 cases of single SPO, six cases of posterior vertebral column resection (PVCR), five cases of PSO + partial pedicle subtraction osteotomy (PPSO), and four cases of PPSO. The mean correction angles were 31.9degrees +/- 11.7degrees with PSO, 14.3degrees +/- 8.4degrees with SPO, 38.3degrees +/- 12.7degrees with PVCR, and 19.3degrees +/- 7.1degrees with PPSO. The thoracolumbar type was the most common. The outcome analysis showed a significant improvement in the ODI score (p < 0.05). Statistical analysis revealed that the ODI score improvements correlated significantly with the postoperative SVA and CCROM (p < 0.05). There was no correlation between the clinical outcomes and spinopelvic parameters. There were 38 surgery-related complications in 25 patients (10.1%).
CONCLUSIONS
Corrective osteotomy is an effective method for treating a fixed kyphotic deformity occurring in ankylosing spondylitis, resulting in satisfactory outcomes with acceptable complications. The CCROM and postoperative SVA were important factors in determining the outcome.
MeSH Terms
Figure
-
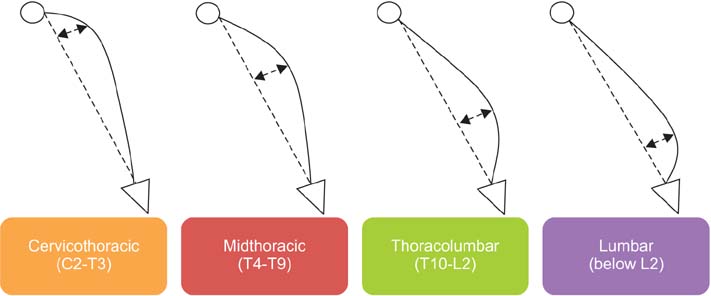
Fig. 1 Type of deformity according to the location of apex.
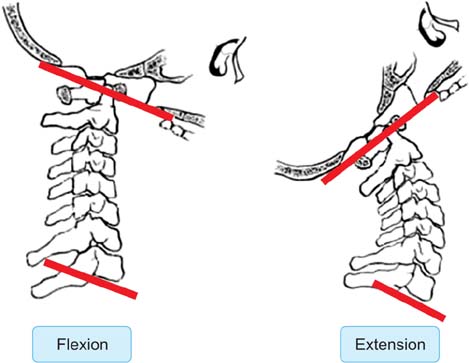
Fig. 2 Diagram of the craniocervical range of motion.
Reference
-
1. Ward MM. Health-related quality of life in ankylosing spondylitis: a survey of 175 patients. Arthritis Care Res. 1999; 12(4):247–255.
Article2. Goel MK. Vertebral osteotomy for correction of fixed flexion deformity of the spine. J Bone Joint Surg Am. 1968; 50(2):287–294.
Article3. Thiranont N, Netrawichien P. Transpedicular decancellation closed wedge vertebral osteotomy for treatment of fixed flexion deformity of spine in ankylosing spondylitis. Spine (Phila Pa 1976). 1993; 18(16):2517–2522.
Article4. Berven SH, Deviren V, Smith JA, Emami A, Hu SS, Bradford DS. Management of fixed sagittal plane deformity: results of the transpedicular wedge resection osteotomy. Spine (Phila Pa 1976). 2001; 26(18):2036–2043.5. Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002; 27(6):612–618.
Article6. Chang KW, Chen YY, Lin CC, Hsu HL, Pai KC. Closing wedge osteotomy versus opening wedge osteotomy in ankylosing spondylitis with thoracolumbar kyphotic deformity. Spine (Phila Pa 1976). 2005; 30(14):1584–1593.
Article7. Hehne HJ, Zielke K, Bohm H. Polysegmental lumbar osteotomies and transpedicled fixation for correction of long-curved kyphotic deformities in ankylosing spondylitis: report on 177 cases. Clin Orthop Relat Res. 1990; (258):49–55.8. Kim WJ. Optimal Standing Radiographic Positioning in Patients with Sagittal Imbalance. J Korean Soc Spine Surg. 2010; 17(4):198–204.
Article9. O'Brien MF, Kuklo TR, Blanke KM, Lenke LG. Radiographic measurement manual. Memphis, TN: Medtronic Sofamor Danek;2008.10. Kim KT, Lee SH, Kwack YH, Son ES. Is it real false negative finding in motor evoked potential monitoring during corrective surgery of ankylosing spondylitis? A case report. Asian Spine J. 2012; 6(1):50–54.
Article11. Lee A. PION after lumbar spine injury. Ophthalmology. 2004; 111(3):612.
Article12. Kim KT, Park DH, Lee SH, Suk KS, Lee JH, Park KJ. Partial pedicle subtraction osteotomy as an alternative option for spinal sagittal deformity correction. Spine (Phila Pa 1976). 2013; 38(14):1238–1243.
Article13. Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine (Phila Pa 1976). 1999; 24(16):1712–1720.
Article14. van Royen BJ, Scheerder FJ, Jansen E, Smit TH. ASKyphoplan: a program for deformity planning in ankylosing spondylitis. Eur Spine J. 2007; 16(9):1445–1449.
Article15. Ondra SL, Marzouk S, Koski T, Silva F, Salehi S. Mathematical calculation of pedicle subtraction osteotomy size to allow precision correction of fixed sagittal deformity. Spine (Phila Pa 1976). 2006; 31(25):E973–E979.
Article16. Van Royen BJ, De Gast A, Smit TH. Deformity planning for sagittal plane corrective osteotomies of the spine in ankylosing spondylitis. Eur Spine J. 2000; 9(6):492–498.
Article17. Kim YJ, Bridwell KH, Lenke LG, Cheh G, Baldus C. Results of lumbar pedicle subtraction osteotomies for fixed sagittal imbalance: a minimum 5-year follow-up study. Spine (Phila Pa 1976). 2007; 32(20):2189–2197.
Article18. Schwab FJ, Patel A, Shaffrey CI, et al. Sagittal realignment failures following pedicle subtraction osteotomy surgery: are we doing enough? Clinical article. J Neurosurg Spine. 2012; 16(6):539–546.
Article19. Schwab F, Lafage V, Patel A, Farcy JP. Sagittal plane considerations and the pelvis in the adult patient. Spine (Phila Pa 1976). 2009; 34(17):1828–1833.
Article20. Yang BP, Ondra SL, Chen LA, Jung HS, Koski TR, Salehi SA. Clinical and radiographic outcomes of thoracic and lumbar pedicle subtraction osteotomy for fixed sagittal imbalance. J Neurosurg Spine. 2006; 5(1):9–17.
Article21. Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010; 35(25):2224–2231.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multisegmental Osteotomy for Kyphotic Deformity in Ankylosing Spondylitis
- Computer Simulation for Surgical Correction of Kyphotic Deformity in Ankylosing Spondylitis: A Narrative Review
- Effect of the Corrective Osteotomy in Ankylosing Spondylitis to Quality of Life(QOL)
- Kyphotic Deformity after Spinal Fusion in a Patient with Diffuse Idiopathic Skeletal Hyperostosis: A Case Report
- The Incidence and Management of Dural Tears and Cerebrospinal Fluid Leakage during Corrective Osteotomy for Ankylosing Spondylitis with Kyphotic Deformity
