Infect Chemother.
2008 Apr;40(2):110-115. 10.3947/ic.2008.40.2.110.
Invasive Aspergillosis of the Paranasal Sinuses Invading Skull Base : Successful Treatment with Voriconazole
- Affiliations
-
- 1Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. heejinmd@medimail.co.kr
- 2Department of Pathology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2230014
- DOI: http://doi.org/10.3947/ic.2008.40.2.110
Abstract
- Skull base-invading, invasive aspergillosis is rare, but it is a potentially life-threatening disease. Nevertheless, the standard method and the optimal duration of treatment are not known yet. A 52-year-old female diabetic patient complained of ophthalmalgia and decreased visual acuity. MRI and CT scan revealed an enhancing mass in the right orbital fissure and showed an infiltrating process in the skull base around the right orbit apex and paranasal sinuses. The histological investigation revealed invasive aspergillosis of paranasal sinuses and the skull base. Clinical improvement occurred after marsupialization and post-operative systemic antifungal therapy with voriconazole for 14 weeks. We suggest that voriconazole treatment could show effective results for invasive aspergillosis of skull base and paranasal sinuses.
Keyword
MeSH Terms
Figure
-
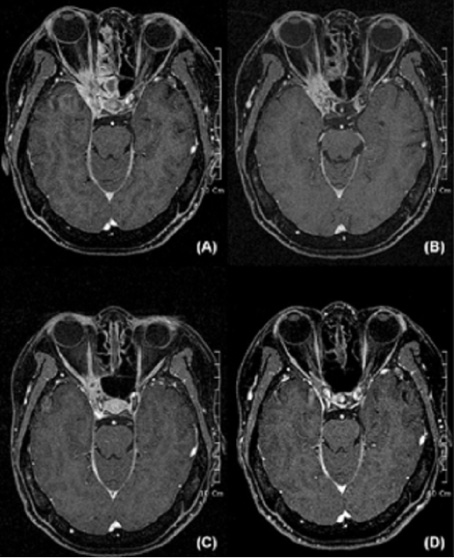
Fig. 1 Posterior Fossa MRI T1WI image shows an enhancing mass like lesion in the right skull base around the superior orbital fissure, anterior middle cranial fossa, around the lateral wall of the right sphenoid sinus, right orbital apex and around the right carvernous sinus: (A) before voriconazole treatment, (B) 4 weeks following voriconazole treatment, (C) at the time of discontinuation of treatment for 14 weeks, and (D) 9 months later from treatment completion.
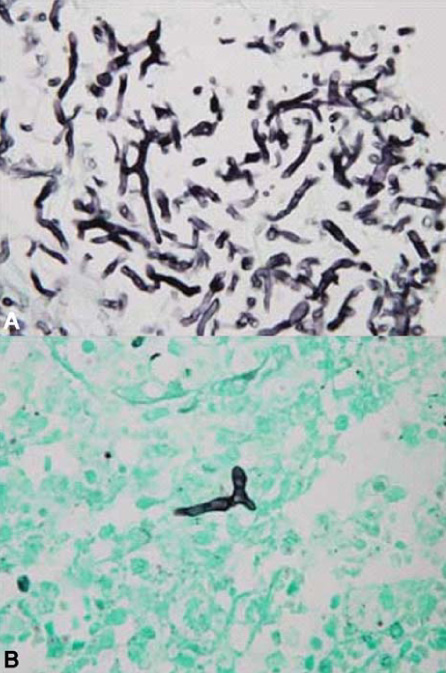
Fig. 2 (A) Specimen from mass of right nasal cavity showing Aspergillosis in Gomori's methenamine-silver (GMS) stain, ×1,000, (B) Slide showing Aspergillus hyphae invading tissue in GMS stain, x1,000.
Reference
-
1. Rinaldi MG. Invasive aspergillosis. Rev Infect Dis. 1983. 5:1061–1077.2. deShazo RD, Chapkin K, Swain RE. Fungal sinusitis. N Engl J Med. 1997. 337:254–259.
Article3. Stevens DA, Kan VL, Judson MA, Morrison VA, Dummer S, Denning DW, Bennett JE, Walsh TJ, Patterson TF, Pankey GA. Practice guidelines for diseases caused by Aspergillus. Infectious Diseases Society of America. Clin Infect Dis. 2000. 30:696–709.
Article4. Lee JY, Kim SB, Kim YH, Kim JH, Yu SK, Kim HY, Jung YK, Park SC, Jung HH, Choi JG, Lee JS, Kim MJ. A Case of invasive aspergillosis of skull base in a diabetic patient. Infect Chemother. 2003. 35:310–314.5. Ryu SY, Chung TI, Han SY, Kim YI, Kim BK. Two cases of invasive aspergillosis of sino-nasal origin. J Korean Neurol Assoc. 2000. 18:368–371.
Article6. Knipping S, Holzhausen HJ, Koesling S, Bloching M. Invasive aspergillosis of the paranasal sinuses and the skull base. Eur Arch Otorhinolaryngol. 2007. 264:1163–1169.
Article7. Kuga A, Oishi K, Ishida H, Kanda F. A case of orbital apex syndrome caused by localized invasive aspergillosis successfully treated with voriconazole. Rinsho Shinkeigaku. 2007. 47:207–210.8. Baumann A, Zimmerli S, Huäsler R, Caversaccio M. Invasive Sphenoidal aspergillosis: successful treatment with sphenoidotomy and voriconazole. ORL J Otorhinolaryngol Relat Spec. 2007. 69:121–126.
Article9. Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature. Clin Infect Dis. 2001. 32:358–366.
Article10. Lionakis MS, Kontoyiannis DP. Fusarium infections in critically ill patients. Semin Respir Crit Care Med. 2004. 25:159–169.11. Perfect JR, Marr KA, Walsh TJ, Greenberg RN, DuPont B, de la Torre-Cisneros J, Just-Näbling G, Schlamm HT, Lutsar I, Espinel-Ingroff A, Johnson E. Voriconazole treatment for less-common, emerging, or refractory fungal infections. Clin Infect Dis. 2003. 36:1122–1131.
Article12. Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, Kern WV, Marr KA, Ribaud P, Lortholary O, Sylvester R, Rubin RH, Wingard JR, Stark P, Durand C, Caillot D, Thiel E, Chandrasekar PH, Hodges MR, Schlamm HT, Troke PF, de Pauw B. Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillys Study Group. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002. 347:408–415.
Article13. Joo YD, Lee WS, Kim JL, Yang JW, Kim HW, Park SK, Sohn CH. A Case of Invasive Maxillary and Orbital Aspergillosis Inhematopoietic Stem Cell Transplantation Recipient with Severe Aplastic Anemia. Korean J Hematol. 2005. 40:205–209.
Article14. Song MJ, Lee DG, Seo SM, Kim WC, Bin HG, Woo HY, Jeon YJ, Cho SG, Son BC, Lee HK. A Case of Fatal Multiple Cerebral Aspergillosis in a Patient with Acute Promyelocytic Leukemia during Complete Remission. Korean J Hematol. 2005. 40:167–171.
Article15. Ahn JH, Kim YJ. Invasive Aspergillosis of the Maxillary Sinus Invading Skull Base : Report of a Case. Korean J Otolaryngol-Head Neck Surg. 1999. 42:652–655.16. Pradhan S, Yadav R. Invasive aspergillosis of the brain: Improvement with lyposomal amphoterecin B and itraconazole. Neurol India. 2007. 55:309–310.
Article17. Gubler C, Wildi SM, Imhof A, Schneemann M, Müllhaupt B. Disseminated invasive aspergillosis with cerebral involvement successfully treated with caspofungin and voriconazole. Infection. 2007. 35:364–366.
Article18. Chopra H, Dua K, Malhotra V, Gupta RP, Puri H. Invasive fungal sinusitis of isolated sphenoid sinus in immunocompetent subjects. Mycoses. 2006. 49:30–36.
Article19. Agarwal S, Kanga A, Sharma V, Sharma DR, Sharma ML. Invasive aspergillosis involving multiple paranasal sinuses: a case report. Indian J Med Microbiol. 2005. 23:195–197.
Article20. Kusaka K, Shimamura I, Ohashi Y, Ota S. Long term survival of patient with invasive aspergillosis involving orbit, paranasal sinus, and central nervous system. Br J Ophthalmol. 2003. 87:791–792.
Article21. Nakamaru Y, Fukuda S, Maguchi S, Takagi D, Inuyama Y. A case of invasive aspergillosis of the paranasal sinuses with a feature of allergic Aspergillus sinusitis. Otolaryngol Head Neck Surg. 2002. 126:204–205.
Article22. Streppel M, Bachmann G, Arnold G, Damm M, Stennert E. Successful treatment of an invasive aspergillosis of the skull base and paranasal sinuses with liposomal amphotericin B and itraconazole. Ann Otol Rhinol Laryngol. 1999. 108:205–207.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Book Review: Endoscopic Surgery of the Paranasal Sinuses and Anterior Skull Base
- Image-Guided Surgery in the Paranasal Sinus and Skull Base Lesion
- Aspergillosis of the paranasal sinuses: diagnostic significance of the computed tomography
- A Case of Invasive Aspergillosis of the Paranasal Sinuses Treated with Surgery and Voriconazole after Kidney Transplantation
- Evolution of the paranasal sinuses' anatomy through the ages
