Severe Stenosis of the Left Main Coronary Artery Detected on Electrophysiologic Study
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea. mdjunkim@yahoo.co.kr
- KMID: 2225850
- DOI: http://doi.org/10.4070/kcj.2008.38.2.119
Abstract
- A cardiac electrophysiologic study (EPS) is a safe procedure with a low complication rate. We report here a case of severe stenosis of the left main coronary artery (LMCA) that was incidentally detected during an EPS; this was successfully managed by stenting the LMCA. The patient was a 75-year-old man with recurrent chest fluttering and no previous angina underwent EPS and he developed acute ischemic chest pain due to induced atrial fibrillation. The coronary angiography showed a critical stenosis in the distal LMCA. The patient underwent percutaneous coronary intervention with a sirolimus-eluting stent in the LMCA. The patient has remained asymptomatic during a 1-year follow-up period. To prevent potentially catastrophic complications, performing a stress myocardial imaging test should be strongly considered before conducting EPS in elderly patients.
MeSH Terms
Figure
-
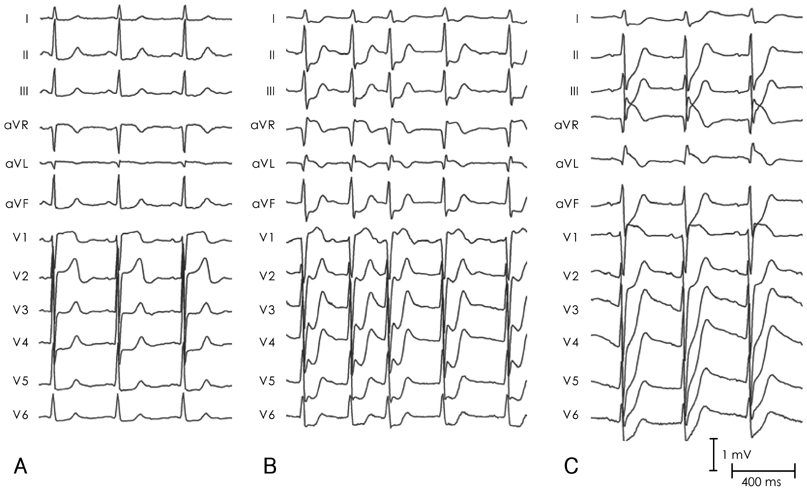
Fig. 1 Standard 12-lead electrocardiograms (ECG) of the patient. The baseline ECG (A) showed non-specific ST-T changes. There was ST segment depression in the precordial and inferior leads during induced atrial fibrillation (B). After cardioversion, there is marked ST segment elevation in leads aVR and V1 in addition to ST segment depression in the precordial and inferior leads (C).
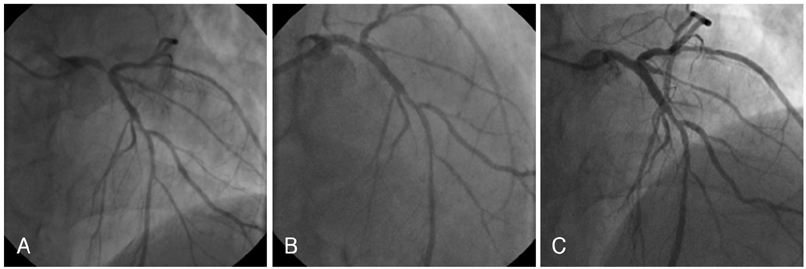
Fig. 2 Coronary angiogram. Left coronary angiogram showing a tight stenosis in the distal left main coronary artery (LMCA) and 50% stenosis at the mid-left anterior descending artery (LAD) (A). There was no residual stenosis after deployment of a sirolimus-eluting stent in the distal LMCA (B). Follow-up coronary angiography after one year showed a patent stent in the LMCA (C).
Reference
-
1. Josephson ME. Electrophysiologic Investigation: Technical Aspects. Clinical Cardiac Electrophysiology Technique and Interpretation. 2002. 3rd. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins;1–18.2. Dimarco JP, Garan H, Ruskin JN. Complications in patients undergoing cardiac electrophysiologic procedures. Ann Intern Med. 1982. 97:490–493.3. Chen SA, Chiang CE, Tai CT, et al. Complications of diagnostic electrophysiologic studies and radiofrequency catheter ablation in patients with tachyarrhythmias: an eight-year survey of 3,966 consecutive procedures in a tertiary referral center. Am J Cardiol. 1996. 77:41–46.4. Gaitonde RS, Sharma N, Ali-Hasan S, Miller JM, Jayachandran JV, Kalaria VG. Prediction of significant left main coronary artery stenosis by the 12-lead electrocardiogram in patients with rest angina pectoris and withholding of clopidogrel therapy. Am J Cardiol. 2003. 92:846–848.5. Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J. Prognostic value of lead aVR in patients with a first non-ST-segment elevation acute myocardial infarction. Circulation. 2003. 108:814–819.6. Yamaji H, Iwasaki K, Kusachi S, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography: ST segment elevation in lead aVR with less ST segment elevation in lead V1. J Am Coll Cardiol. 2001. 38:1348–1354.7. Hirano T, Tsuchiya K, Nishigaki K, et al. Clinical features of emergency electrocardiography in patients with myocardial infarction caused by left main trunk obstruction. Circ J. 2006. 70:525–529.8. Park SJ, Kim YH, Lee BK, et al. Sirolimus-eluting stent implantation for unprotected left main coronary artery stenosis: comparison with bare metal stent implantation. J Am Coll Cardiol. 2005. 45:351–356.9. Park SJ, Park SW, Hong MK, et al. Long-term (three-year) outcomes after stenting of uprotected left main stenosis in patients with normal left ventricular function. Am J Cardiol. 2003. 91:12–16.10. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation. 2004. 110:e340–e437.11. Lee SW, Hong MK, Kim YH, et al. Bail-out stenting for left main coronary artery dissection during catheter-based procedure: acute and long-term results. Clin Cardiol. 2004. 27:393–395.12. Park JH, Cho YH, Lee SW, et al. Long-term clinical follow-up in patients with left main coronary disease according to treatment strategies. Korean Circ J. 2003. 33:568–573.13. Park SJ, Park SW, Hong MK, et al. Stenting of unprotected left main coronary artery stenosis without anticoagulation: immediate and late outcomes. Korean Circ J. 1997. 27:947–957.14. Schwartz JB, Zipes DP. Zipes DP, editor. Cardiovascular disease in the elderly. Braunwald's Heart Disease: A Textbook Of Cardiovascular Medicine. 2005. 7th. Philadelphia, Pennsylvania: Elsevier Saunders;1925–1949.15. Coleman KA, Steingart RM, Pollack S, Cohen TJ. Utility of stress myocardial perfusion imaging performed before electrophysiologic testing. J Nucl Cardiol. 2003. 10:676–683.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Ostial left Main Stenosis Diagnosed by Transesophageal Doppler Echocardiography
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
- Isolated Coronary Ostial Stenosis Confirmed by Transesophageal Echocardiogram: A Case Report
- The Clinical Experiences of Patch Angioplasty in Isolated Critical Left Main Coronary Artery Stenosis
- A Case of Left Coronary Osteal Stenosis Combined with Moyamoya Disease
