Two Cases of Successful Primary Percutaneous Coronary Intervention in Patients With an Anomalous Right Coronary Artery Arising From the Left Coronary Cusp
- Affiliations
-
- 1Department of Internal Medicine, Vision 21 Cardiac and Vascular Center, Korea. djh95@ilsanpaik.ac.kr
- 2Clinical Research Center, Ilsan-Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- KMID: 2225836
- DOI: http://doi.org/10.4070/kcj.2008.38.3.179
Abstract
- An anomalous origin of the right coronary artery (RCA) from the left coronary cusp is a rare congenital anomaly. Because of the unusual location and the noncircular luminal orifice of this anomaly, cannulation of this artery during coronary angiography and percutaneous coronary intervention (PCI) poses significant technical difficulties when using the currently available guiding catheters. Primary PCI should be performed as quickly as possible when a patient displays this condition. When we face the situation of an anomalous artery during primary PCI, it takes a much longer time to open the occluded artery. We report here on two cases of successful primary PCI with using manually manipulated catheters and Ikari type guiding catheters in 2 patients who both had an anomalous RCA arising from the left coronary cusp.
Keyword
MeSH Terms
Figure
-
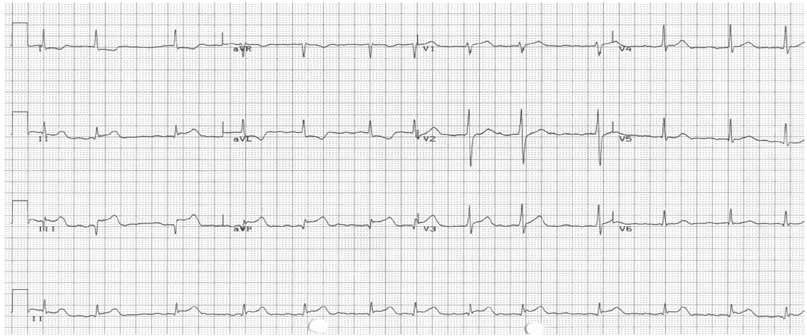
Fig. 1 An electrocardiogram showed ST segment elevation in the II, III and aVF leads.
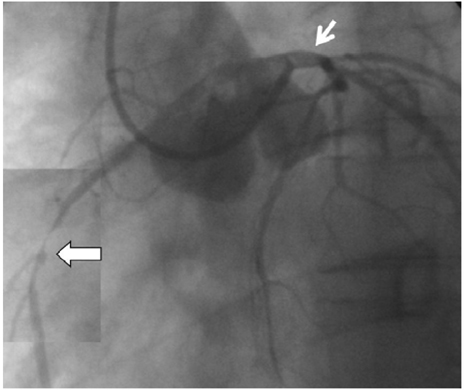
Fig. 2 Baseline coronary angiogram showed an anomalous right coronary artery (RCA) ostium (small arrow) and subtotal occlusion of the mid-RCA (large arrow).
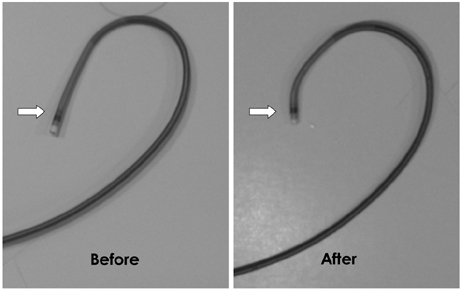
Fig. 3 5 French launcher EBU4 guiding catheter. Before: the natural shape of the EBU4 guiding catheter. After: the manually manipulated EBU4 guiding catheter (arrow) using a hair dryer. EBU: extra-backup.
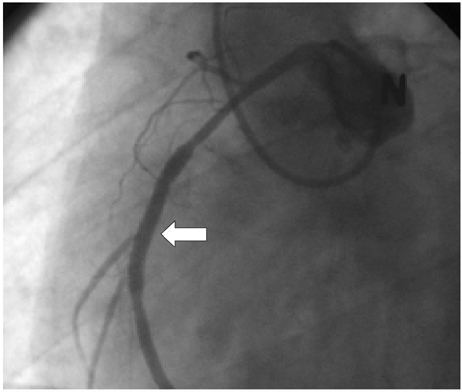
Fig. 4 The final coronary angiogram showed a successfully implanted stent at the mid right coronary artery (arrow).
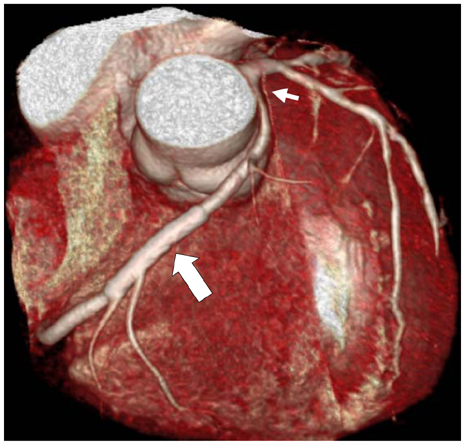
Fig. 5 The 64 slice multi-detector computed tomography (MDCT) showed an anomalous right coronary artery ostium (small arrow) and patent stent lumen (large arrow).
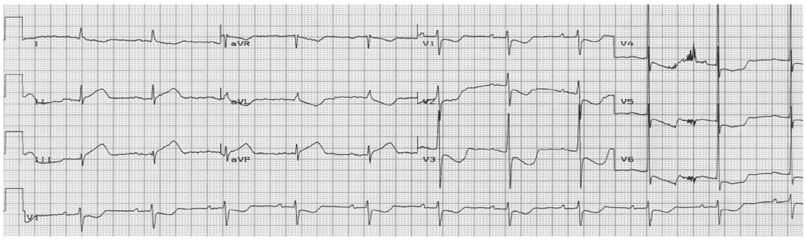
Fig. 6 An electrocardiogram showed ST segment elevation in the II, III and aVF leads.

Fig. 7 A: baseline coronary angiogram using a 6 French Heartrail Ikari right 1.5 guiding catheter showed an anomalous right coronary artery (RCA) ostium (small arrow) and total occlusion of the distal RCA (large arrow). B: 6 French Heartrail Ikari right 1.5 guiding catheter.
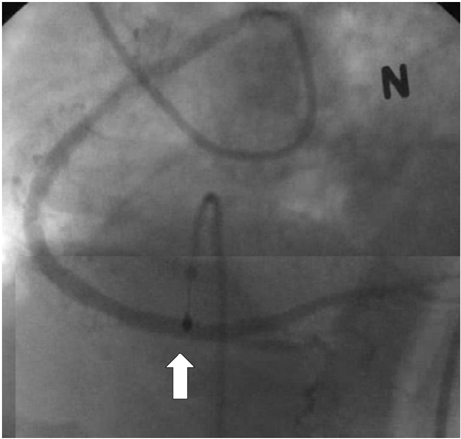
Fig. 8 The final coronary angiogram showed a successfully implanted stent at the distal right coronary artery (arrow).
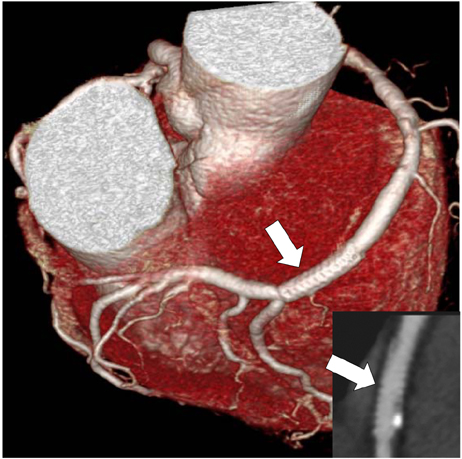
Fig. 9 The 64 slice multi-detector computed tomography showed a patent stent lumen (arrows).
Reference
-
1. Kimbris D, Iskanderian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978. 58:606–615.2. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary angiography. Cathet Cardiovasc Diagn. 1990. 21:28–40.3. Rigatelli G, Docali G, Rossi P, et al. Congenital coronary artery anomalies angiographic classification revisited. Int J Cardiovasc Imaging. 2003. 19:361–366.4. Garcia-Rinaldi R, Sosa J, Olmeda S, Cruz H, Carballido J, Quintana C. Surgical treatment of right coronary arteries with anomalous origin and slit ostium. Ann Thorac Surg. 2004. 77:1525–1529.5. Benge W, Martins J, Funk DC. Morbidity associated with anomalous origin of the right coronary artery from the left sinus of valsalva. Am Heart J. 1980. 99:96–100.6. Isner JM, Shen EM, Martin ET, Fortin RV. Sudden unexpected death as a result of anomalous origin of the right coronary artery from the left sinus of valsalva. Am J Med. 1984. 76:155–158.7. Spargias K, Kariofyllis P, Mavrogeni S. Percutaneous coronary intervention in anomalous right coronary arteries arising from the left sinus of valsalva: a report of two cases and observations on the pattern of atherosclerosis. J Invasive Cardiol. 2006. 18:E78–E81.8. Choi KL, Kwon JI, Jung WH, et al. Stenting of an anomalous coronary artery in acute myocardial infarction. Korean Circ J. 1998. 28:1378–1381.9. Cha KS, Keum DJ, Park HR, et al. Transradial stenting of an anomalous right coronary artery originating from the left sinus of valsalva. Korean Circ J. 1998. 28:2056–2060.10. Topaz O, DiSciascio G, Gondreau E, et al. Coronary angioplasty of anomalous of coronary arteries: notes on technical aspects. Cathet Cardiovasc Diagn. 1990. 21:106–111.11. Qayyum U, Leya F, Steen L, et al. New catheter design for cannulation of the anomalous right coronary artery arising from the left sinus of valsalva. Catheter Cardiovasc Interv. 2003. 60:382–388.12. Cohen MG, Tolleson TR, Peter RH, Harrison JK, Sketch MH Jr. Successful percutaneous coronary intervention with stent implantation in anomalous right coronary arteries arising from the left sinus of valsalva: a report of two cases. Catheter Cardiovasc Interv. 2002. 55:105–108.13. Oral D, Dagalp Z, Pamir G, et al. Percutaneous transluminal coronary angioplasty of anomalous coronary arteries: case reports. Angiology. 1996. 47:77–82.14. Lorin JD, Robin B, Lochow P, Lorenzo A, Sedlis SP. The right radial approach for stenting of lesions in the right coronary artery with anomalous take-off from the left sinus of valsalva. J Invasive Cardiol. 2000. 12:478–480.15. Ikari Y, Nakajima H, Iijima R, et al. Initial characterization of Ikari Guide catheter for transradial coronary intervention. J Invasive Cardiol. 2004. 16:65–68.16. Sato Y, Ichikawa M, Masubuchi M, et al. MDCT of the anomalous origin of the right coronary artery from the left sinus of valsalva as a single coronary artery. Int J Cardiol. 2006. 109:125–126.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
- Anomalous Origin of the Left Coronary Artery from the Right Sinus of Valsalva, which Presented as Acute Myocardial Infarction
- Transradial Stenting of an Anomalous Right Coronary Artery Originating from the Left Sinus of Valsalva
- Anomalous Origin of the Right Coronary Artery from the Left Anterior Descending Artery: An Extremely Rare Variety of Single Coronary Artery
- Congenital Absence of Left Circumflex Coronary Artery: Circumflex Artery Extended from Right Coronary Artery
