The Measurement of Opening Angle and Orifice Area of a Bileaflet Mechanical Valve Using Multidetector Computed Tomography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. younhj@catholic.ac.kr
- 2Department of Thoracic Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2225691
- DOI: http://doi.org/10.4070/kcj.2009.39.4.157
Abstract
- BACKGROUND AND OBJECTIVES
The aim of this study was to assess mechanical valve function using 64-slice multidetector computed tomography (MDCT). SUBJECTS AND METHODS: In 20 patients (mean age, 50+/-12 years; male-to-female ratio, 10:10), 30 St. Jude bileaflet mechanical valves (15 aortic and 15 mitral valves) were evaluated using MDCT. We selected images vertical and parallel to the mechanical valve. The valve orifice area (OA) and valve length were determined by manual tracing and the opening and closing angles were measured using a protractor. The OA and length of the mechanical valves were compared with the manufacturer's values. RESULTS: The geometric orifice areas (GOAs) based on the manufacturer's values and the OAs determined by MDCT were 3.4+/-0.2 cm2 and 3.4+/-0.3 cm2 for the mitral valves and 2.1+/-0.3 cm2 and 2.1+/-0.4 cm2 for the aortic valves, respectively. The correlation coefficients between the OA measures were 0.433 for the mitral valves and 0.874 for the aortic valves (both p<0.001). The lengths based on the manufacturer's values and determined by MDCT were 29.3+/-1.99 mm and 29.6+/-1.65 mm for the mitral valves and 21.5+/-2.1 mm and 20.7+/-2.3 mm for the aortic valves, respectively. The correlation coefficients between the measures were 0.651 for the mitral valve and 0.846 for the aortic valve (both p<0.001). The opening and closing angles determined by MDCT were 10.9+/-0.6degrees and 131.1+/-3.2degrees for the mitral valves and 11.1+/-0.9degrees and 120.6+/-1.7degrees for the aortic valves, respectively. CONCLUSION: MDCT is an accurate modality with which to assess the function and morphology of bileaflet mechanical valves.
Keyword
Figure
-
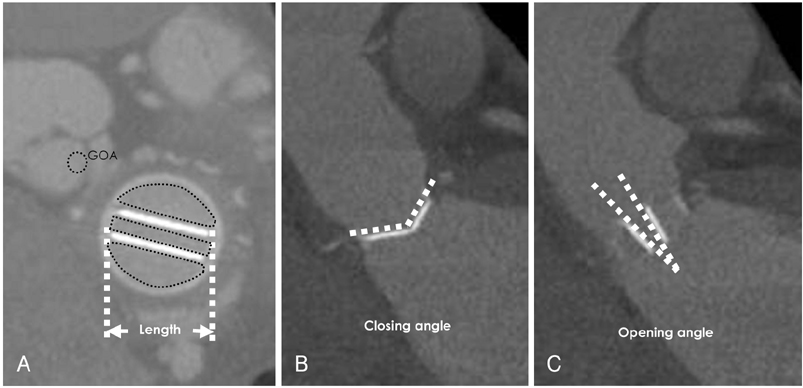
Fig. 1 The GOAs, lengths, and opening/closing angles of SJM valves determined by 64-slice MDCT. The images are analyzed using an Image-Pro Plus Image module (Media Cybernetics) and were compared with the manufacturer's values for the GOAs, lengths (A), opening angles (B), and closing angles (C) of the SJM valves as determined by 64-slice MDCT. GOAs and lengths were measured on the vertical image of the mechanical valve. The opening and closing angles were measured on parallel images of the mechanical valve. GOA: geometric orifice area, SJM: St. Jude Medical, MDCT: multidetector computed tomography.
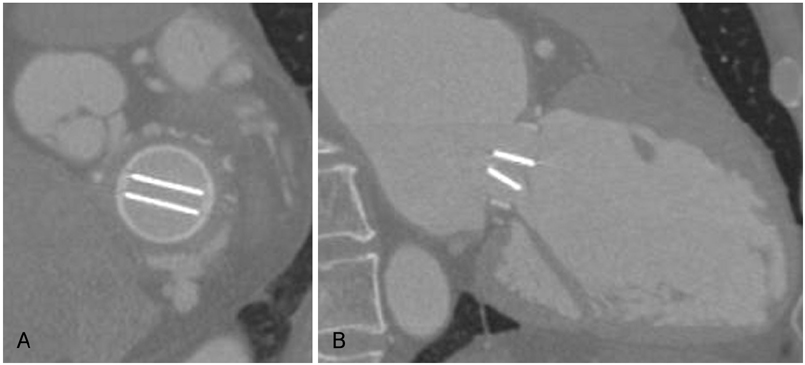
Fig. 2 A 39-year-old woman who presented for assessment of function after undergoing SJM mitral valve replacement (valve size, 29 mm) for infective endocarditis. In the mitral valve, the GOA determined by MDCT was 3.35 cm2 and the manufacturer's value was 3.5 cm2. The valve length determined by MDCT was 28.6 mm and the manufacturer's value was 29 mm. The opening angle determined by MDCT was 11.2° and the manufacturer's value was 10°, and the closing angle determined by MDCT was 132.1° and the manufacturer's value was 130°. A: a vertical reformatted image of the valve shows the SJM mitral valve (#29) with symmetric opening of mechanical components. The valve is intact, based on measurement of the GOA and the length. B: a parallel reformatted image of valve shows the SJM mitral valve (#29). The valve is intact based on measurement of the opening and closing (not shown) angles. SJM: St. Jude Medical, GOA: geometric orifice area, MDCT: multidetector computed tomography.
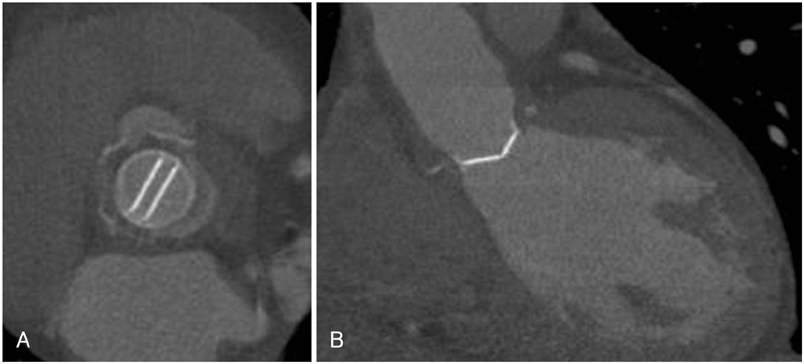
Fig. 3 A 54-year-old woman who presented for assessment of function after undergoing SJM aortic valve replacement (valve size, 19 mm) for severe aortic stenosis. In the aortic valve, the GOA determined by MDCT was 1.68 cm2 and the manufacturer's value was 1.7 cm2. The valve length determined by MDCT was 18.6 mm and the manufacturer's value was 19 mm. The opening angle determined by 64-slice MDCT was 11.7° and the manufacturer's value was 10°, and the closing angle determined by MDCT was 119.6° and the manufacturer's value was 120°. A: a vertical reformatted image of valve shows the SJM aortic valve (#29) with symmetric opening of the mechanical components. The valve is intact based on measurement of the GOA and the length. B: a parallel reformatted image of valve shows the SJM aortic valve (#29) with symmetric opening of the mechanical components. The valve is intact based on measurement of the opening (not shown) and closing angles. SJM: St. Jude Medical, GOA: geometric orifice area, MDCT: multidetector computed tomography.
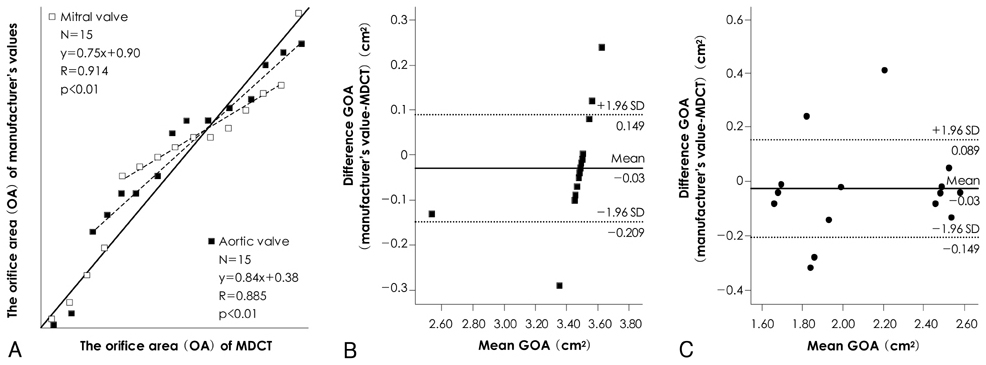
Fig. 4 The correlation coefficients and Bland-Altman analysis for the GOA based on the manufacturer's value and determined by 64-slice MDCT. A: the correlation coefficients for the GOA based on the manufacturer's value compared with those determined by MDCT were 0.433 for the mitral valve and 0.874 for the aortic valve (p<0.001). B: the Bland-Altman analysis of bias revealed that there were no significant bias between the GOA based on the manufacturer's value and MDCT for the mitral valve (observed bias, 1.121; 95% confidence interval, 0.823-1.1418). C: the Bland-Altman analysis of bias revealed that there were no significant bias between the GOA based on the manufacturer's value and MDCT for the aortic valve (observed bias, 0.938; 95% confidence interval, 0.642-1.223; p<0.001). The solid line is the mean difference; the dotted lines mark the standard deviations of the differences. Mean GOA=(manufacturer's value+MDCT)/2. GOA: geometric orifice area, MDCT: multidetector computed tomography.

Fig. 5 The correlation coefficients and Bland-Altman analysis for the valve length based on the manufacturer's value and determined by 64-slice MDCT. A: the correlation coefficients for the valve lengths based on the manufacturer's values compared with those determined by MDCT were 1.145 for the mitral valve and 0.790 for the aortic valve (p<0.001). B: the Bland-Altman analysis of bias revealed that there was no significant bias between the GOA based on the manufacturer's value and MDCT for the mitral valve (observed bias, 1.121; 95% confidence interval, 0.823-1.1418). C: the Bland-Altman analysis of bias revealed that there was no significant bias between the GOA based on the manufacturer's value and MDCT for the aortic valve (observed bias, 0.938; 95% confidence interval, 0.642-1.223; p<0.001). The solid line is the mean difference; the dotted lines mark the standard deviations of the differences. Mean length GOA=(manufacturer's value+MDCT)/2. GOA: geometric orifice area, MDCT: multidetector computed tomography.
Reference
-
1. Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002. 15:167–184.2. Chambers J, Deverall P. Limitations and pitfalls in the assessment of prosthetic valves with Doppler ultrasonography. J Thorac Cardiovasc Surg. 1992. 104:495–501.3. Muratori M, Montorsi P, Teruzzi G, et al. Feasibility and diagnostic accuracy of quantitative assessment of mechanical prostheses leaflet motion by transthoracic and transesophageal echocardiography in suspected prosthetic valve dysfunction. Am J Cardiol. 2006. 97:94–100.4. Montorsi P, De Bernardi F, Muratori M, Cavoretto D, Pepi M. Role of cine-fluoroscopy, transthoracic, and transesophageal echocardiography in patients with suspected prosthetic heart valve thrombosis. Am J Cardiol. 2000. 85:58–64.5. Koo SH, Kim SH, Oh SI, et al. Echocardiographic characteristics of normally functioning CarboMedics and St. Jude medical mitral valve. Korean Circ J. 1995. 25:469–476.6. Koo SH, Sung JD, Park SS, et al. Clinical utility of transesophageal echocardiography (TEE) in prosthetic valve dysfunction. Korean Circ J. 1993. 23:928–938.7. Kim YN, Song YS, Kim KS, Kim KB, Huh SH, Choi SY. Evaluation of functional regurgitation flow in patients with clinically normal mitral prosthesis by transesophageal echocardiography. Korean Circ J. 1993. 23:67–74.8. Joo SJ, Hyon MS, Doh MH, et al. Changes of Doppler echocardiographic findings after mitral valve operation. Korean Circ J. 1987. 17:649–660.9. Achenbach S, Ulzheimer S, Baum U, et al. Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation. 2000. 102:2823–2828.10. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography with multi-slice computed tomography. Lancet. 2001. 357:599–603.11. Achenbach S, Giesler T, Ropers D, et al. Detection of coronary artery stenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation. 2001. 103:2535–2538.12. Mollet NR, Cademartiri F, van Mieghem CA, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005. 112:2318–2323.13. Becker CR, Kleffel T, Crispin A, et al. Coronary artery calcium measurement: agreement of multirow detector and electron beam CT. AJR Am J Roentgenol. 2001. 176:1295–1298.14. Schuijf JD, Bax JJ, Salm LP, et al. Noninvasive coronary imaging and assessment of left ventricular function using 16-slice computed tomography. Am J Cardiol. 2005. 95:571–574.15. Groen JM, Greuter MJ, van Ooijen PM, Oudkerk M. A new approach to the assessment of lumen visibility of coronary artery stent at various heart rates using 64-slice MDCT. Eur Radiol. 2007. 17:1879–1884.16. Rixe J, Achenbach S, Ropers D, et al. Assessment of coronary artery stent restenosis by 64-slice multi-detector computed tomography. Eur Heart J. 2006. 27:2567–2572.17. Muhlenbruch G, Mahnken AH, Das M, et al. Evaluation of aortocoronary bypass stents with cardiac MDCT compared with conventional catheter angiography. AJR Am J Roentgenol. 2007. 188:361–369.18. Jones CM, Athanasiou T, Dunne N, et al. Multi-detector computed tomography in coronary artery bypass graft assessment: a meta-analysis. Ann Thorac Surg. 2007. 83:341–348.19. Ropers D, Pohle FK, Kuettner A, et al. Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation. 2006. 114:2334–2341.20. Salm LP, Bax JJ, Jukema JW, et al. Comprehensive assessment of patients after coronary artery bypass grafting by 16-detector-row computed tomography. Am Heart J. 2005. 150:775–781.21. Hoffmann U, Ferencik M, Cury RC, Pena AJ. Coronary CT angiography. J Nucl Med. 2006. 47:797–806.22. Dawson P. Multi-slice CT contrast enhancement regimens. Clin Radiol. 2004. 59:1051–1060.23. Willmann JK, Kobza R, Roos JE, et al. ECG-gated multi-detector row CT for assessment of mitral valve disease: initial experience. Eur Radiol. 2002. 12:2662–2669.24. Willmann JK, Weishaupt D, Lachat M, et al. Electrocardiographically gated multi-detector row CT for assessment of valveular morphology and calcification in aortic stenosis. Radiology. 2002. 225:120–128.25. Budoff MJ, Cohen MC, Garcia MJ, et al. ACCF/AHA clinical competence statement on cardiac imaging with computed tomography and magnetic resonance. Circulation. 2005. 112:598–617.26. Chiang SJ, Tsao HM, Wu MH, et al. Anatomic characteristics of the left atrial isthmus in patients with atrial fibrillation: lessons from computed tomographic images. J Cardiovasc Electrophysiol. 2006. 17:1274–1278.27. Cury RC, Abbara S, Schmidt S, et al. Relationship of the esophagus and aorta to the left atrium and pulmonary veins: implications for catheter ablation of atrial fibrillation. Heart Rhythm. 2005. 2:1317–1323.28. Schwartzman D, Lacomis J, Wigginton WG. Characterization of left atrium and distal pulmonary vein morphology using multidimensional computed tomography. J Am Coll Cardiol. 2003. 41:1349–1357.29. Hunold P, Vogt FM, Schmermund A, et al. Radiation exposure during cardiac CT: effective doses at multi-detector row CT and electron-beam CT. Radiology. 2003. 226:145–152.30. Morin RL, Gerber TC, McCollough CH. Radiation dose in computed tomography of the heart. Circulation. 2003. 107:917–922.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Measurement of Opening and Closing Angles of Aortic Valve Prostheses In Vivo Using Dual-Source Computed Tomography: Comparison with Those of Manufacturers' in 10 Different Types
- Escape of Mechanical Valve: A case report
- In vitro pressure drop comparison between two mechanical valve prostheses
- Measurement of the so-called "Nasal Valve" in Japanese Subjects
- Transesophageal Doppler Echocardiography in the Evaluation of Mitral Bileaflet Mechanical Prostheses: Comparative Studies between Sorin Bicarbon and ATS Valve Prostheses in Mitral Valve Replacement
