Takayasu's Arteritis Involving the Ostia of Three Large Coronary Arteries
- Affiliations
-
- 1Department of Internal Medicine/Cardiac Catheterization Laboratory, Pusan National University Hospital, Busan, Korea. glaraone@hanmail.net
- KMID: 2225645
- DOI: http://doi.org/10.4070/kcj.2009.39.12.551
Abstract
- Takayasu's arteritis can involve the ostia of coronary arteries. We report a patient with Takayasu's arteritis involving the ostia of three large coronary arteries who was successfully treated by percutaneous coronary intervention (PCI) with a drug-eluting stent (DES) and had a good clinical outcome after 12 months. A 37-year-old male with unstable angina was admitted to our cardiovascular center. The patient had Takayasu's arteritis and an aortic valve replacement with a metallic valve due to severe aortic regurgitation 7 years previously. Coronary angiography (CAG) showed a 95% discrete eccentric luminal narrowing at the ostia of the large left anterior descending (LAD) and left circumflex (LCX) arteries, and a 99% discrete eccentric luminal narrowing at the ostium of the large right coronary artery (RCA). The patient was treated with prednisolone for 14 days. Two large paclitaxel-eluting stents (PES) were then implanted in the distal left main coronary artery using the kissing stent technique. After 6 months, a CAG did not reveal restenosis or recurrent coronary artery disease. Thus, PCI with a DES for patients with significant coronary involvement secondary to Takayasu's arteritis is an effective and an alternative treatment when coronary bypass grafting is not option.
Keyword
MeSH Terms
Figure
-
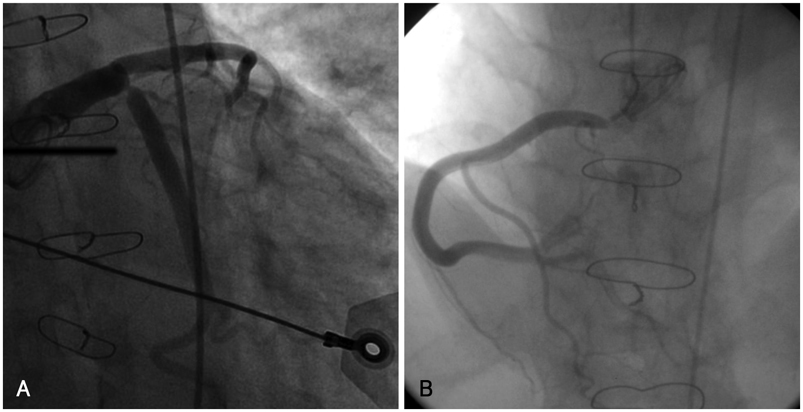
Fig. 1 Initial coronary angiography. A: selective left coronary angiography shows 95% discrete eccentric luminal narrowing at the ostium of the large LAD and large LCX. B: selective right coronary angiography shows 99% discrete eccentric luminal narrowing at the ostium of the large RCA. LAD: left anterior descending, LCX: left circumflex, RCA: right coronary artery.

Fig. 2 Angiography of systemic vessels. A and B: right and left subclavian arteries reveal total occlusion. C: ostium of the right renal artery shows 80% luminal narrowing. D: right superficial femoral artery shows total occlusion with collateral flow.
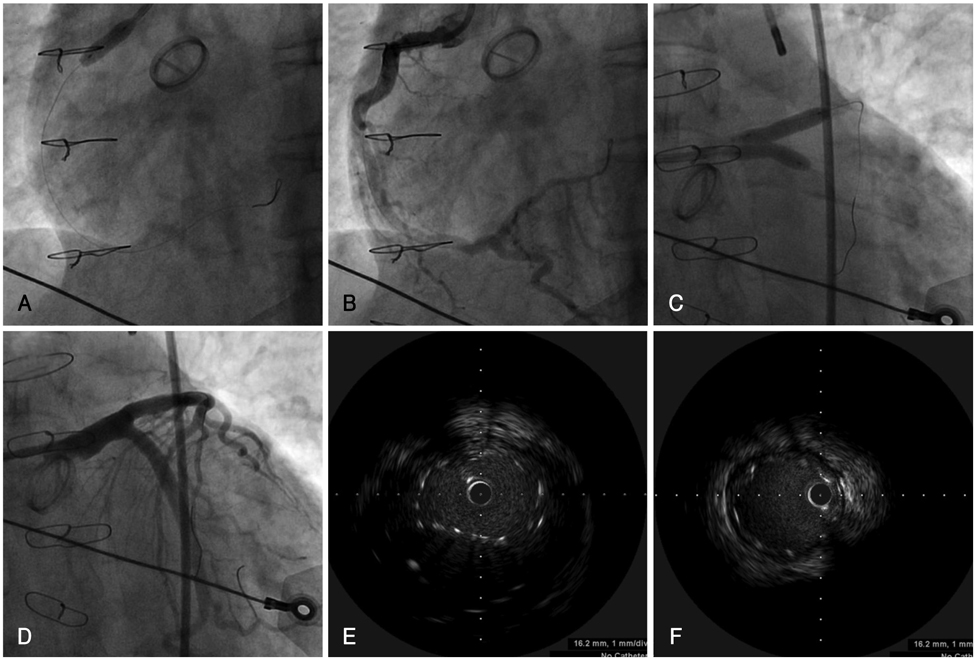
Fig. 3 Coronary angiography (A-D) and IVUS (E and F) during PCI. A and B: a large 5.0×12 mm paclitaxel-eluting stent is implanted in the ostium of the RCA. C and D: two large paclitaxel-eluting stents are implanted from the distal left main coronary artery to the LAD and LCX by the kissing stent technique (LAD: 5.0 mm×24 mm at 14 atm, LCX; 5.0×16 mm at 14 atm). E and F: IVUS show good apposition of kissing stents minimally overlapped from the distal left main coronary artery to the LAD and LCX. RCA: right coronary artery, LAD: left anterior descending, LCX: left circumflex, IVUS: Intravascular ultrasound, PCI: percutaneous coronary intervention.
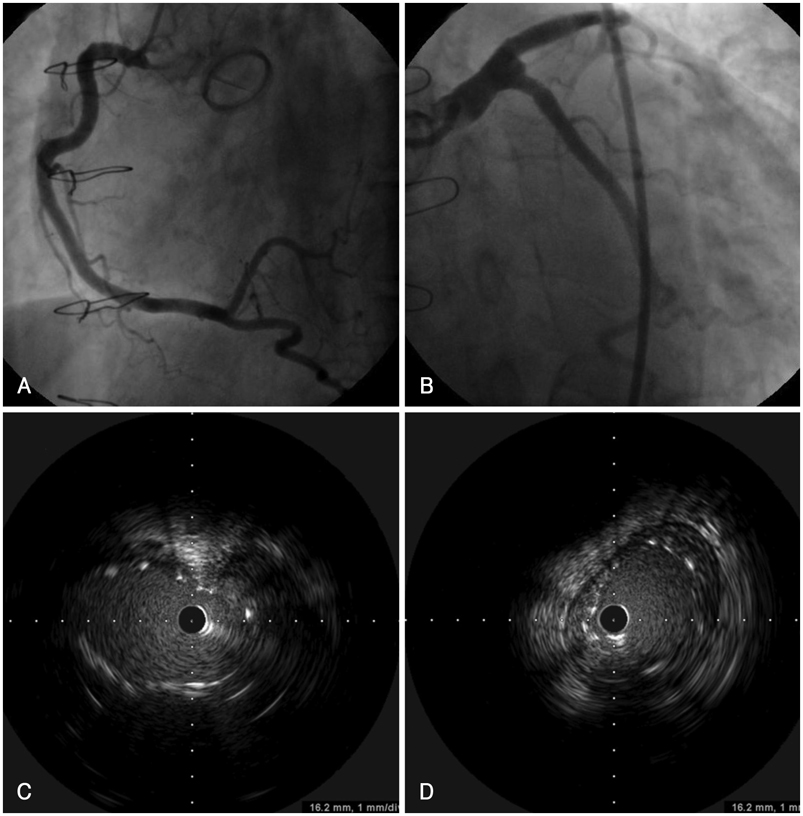
Fig. 4 Follow up coronary angiography (A and B) and IVUS (C and D). A and B: coronary angiography does not show restenosis or recurrence of coronary artery disease in LAD, LCX, and RCA. C and D: IVUS shows little neointimal proliferation and stent malapposition in the distal part of the LAD stent. LAD: left anterior descending, LCX: left circumflex, RCA: right coronary artery, IVUS: Intravascular ultrasound.
Reference
-
1. Furukawa Y, Tamura T, Toma M, et al. Sirolimus-eluting stent for in-stent restenosis of left main coronary artery in takayasu arteritis. Circ J. 2005. 69:752–755.2. Amir O, Kar B, Civitello AB, Palanichamy N, Shakir A, Delgado RM 3rd. Unprotected left main stent placement in a patient with Takayasu's arteritis: an unusual solution for an unusual disease. Tex Heart Inst J. 2006. 33:253–255.3. Kang WC, Han SH, Oh KJ, Ahn TH, Shin EK. Images in cardiovascular medicine: implantation of a drug-eluting stent for the coronary artery stenosis of Takayasu arteritis: de novo and instent restenosis. Circulation. 2006. 113:e735–e737.4. Amano J, Suzuki A. Coronary artery involvement in Takayasu's arteritis: collective review and guideline for surgical treatment. J Thorac Cardiovasc Surg. 1991. 102:554–560.5. Endo M, Tomizawa Y, Nishida H, et al. Angiographic findings and surgical treatments of coronary artery involvement in Takayasu arteritis. J Thorac Cardiovasc Surg. 2003. 125:570–577.6. Son JW, Koh KK, Dang Q, Choi IS, Shin EK. Recurrent restenosis following stent and rotational atherectomy of coronary artery stenosis in Takayasu's arteritis. Int J Cardiol. 1998. 65:295–300.7. Malik IS, Harare O, AL-Nahhas A, Beatt K, Mason J. Takayasu's arteritis: management of left main stem stenosis. Heart. 2003. 89:e9.8. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu's disease). Circulation. 1989. 80:429–437.9. Park YB, Hong SK, Choi KJ, et al. Takayasu arteritis in Korea: clinical and angiographic features. Heart Vessels Suppl. 1992. 7:55–59.10. Matsubara O, Kuwata T, Nemoto T, Kasuga T, Numano F. Coronary artery lesions in Takayasu arteritis: pathological considerations. Heart Vessels Suppl. 1992. 7:26–31.11. Amano J, Suzuki A. Coronary artery involvement in Takayasu's arteritis: collective review and guideline for surgical treatment. J Thorac Cardiovasc Surg. 1991. 102:554–560.12. Amano J, Suzuki A. Surgical treatment of cardiac involvement in Takayasu arteritis. Heart Vessels Suppl. 1992. 7:168–178.13. Chun KJ, Kim SI, Na MA, Choi JH. Bilateral ostial coronary artery lesions in a patient with Takayasu's arteritis. Korean Circ J. 2004. 34:118–119.14. Kang KT, Jeong MH, Jeong WG, et al. Long-term clinical follow-up in a case of Takayasu's arteritis involving the ostium of left coronary artery after ostioplasty. Korean Circ J. 2001. 31:246–250.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Hypertension with Pulmonary Arteritis Diagnosed as Takayasu's Arteritis Type IV
- A Case of Bilateral Coronary Ostial Stenosis in Takayasu's Arteritis
- A Case of Takayasu's Arteritis with Bilateral Involvement of Ostial Coronary Arteries
- Takayasu's Arteritis with Ischemic Stroke Followed by Subarachnoid Hemrrhage: A Case Report
- A Case of Takayasu's Arteritis Associated with Aortic Regurgitation and Coronary Artery Involvement
