Simple Method of Counterclockwise Isthmus Conduction Block by Comparing Double Potentials and Flutter Cycle Length
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Research Institute of Clinical Medicine, Chonbuk National University, Jeonju, Korea.
- 2Department of Preventive Medicine, Research Institute of Clinical Medicine, Chonbuk National University, Jeonju, Korea.
- 3Division of Cardiology, Asan Medical Center, University of Ulsan, Seoul, Korea. kjchoi@amc.seoul.kr
- KMID: 2225640
- DOI: http://doi.org/10.4070/kcj.2009.39.12.525
Abstract
- BACKGROUND AND OBJECTIVES
Local wide split double potentials are used as a parameter to determine complete conduction block during cavotricuspid isthmus ablation in patients with isthmus dependent atrial flutter. However, delayed slow conduction in that region can sometimes be very difficult to differentiate from complete block. Flutter cycle length (FCL) can be used to confirm isthmus conduction block, because FCL is a measure of conduction time around the tricuspid annulus (TA). This study was designed to determine which degree of splitting of the local electrograms is adequate to confirm complete isthmus block, using FCL as a reference. SUBJECTS AND METHODS: Cavotricuspid isthmus (CTI) ablation was performed in fifty consecutive patients. The interval between the pacing stimulus on the lateral side of the CTI and the first component of the double potentials on the block line (SD1) corresponded to the counterclockwise conduction time. The interval between the pacing stimulus and second component (SD2) represented the clockwise conduction time to the contralateral side of the ablation line. SD1 and SD2 were measured before and after complete isthmus block. RESULTS: An SD1+SD2 reaching 90% of the FCL identified the counterclockwise isthmus conduction block with 94% sensitivity and 100% specificity. CONCLUSION: If the sum of SD1 and SD2 following isthmus ablation was close to the FCL, complete conduction block was predicted with high diagnostic accuracy and positive predictive value for at least counterclockwise conduction.
Figure
-

Fig. 1 Displayed from the top, surface ECG leads I, aVF and V1, and intracardiac electrograms from a duodecapolar halo-type 19, 20 to 1, 2 from proximal to distal electrodes located in the right atrium around the tricuspid annulus, and ABLd: ablation catheter. A: wide splitting of the local double potentials (129 ms) is seen in the recording from ABLd, and the activation sequence from the halo-type catheter suggests counterclockwise conduction block of isthmus. B: while waiting following the ablation procedure, the activation sequence of the septal (proximal) electrodes on the halo-type catheter changed, suggesting re-conduction of the isthmus. Local double potentials became narrower, but still the interval between them was almost 110 ms, which is known as a specific indicator of complete isthmus block. C and D: left anterior oblique and right anterior oblique fluoroscopic view of the halo-type and ablation catheter. ECG: electrocardiogram.
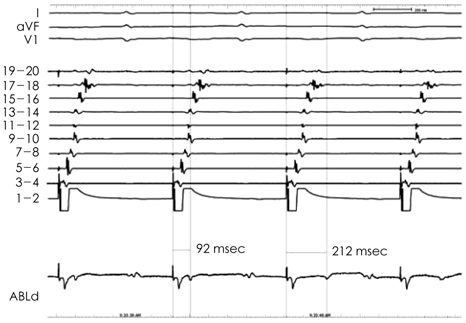
Fig. 2 Complete conduction block was achieved, and was associated with a sudden wide splitting of the local double potentials in the ABLd recording (the third beat). The activation sequence on the halo-type catheter suggests counterclockwise conduction block of the isthmus in all four paced beats, even before achievement of complete isthmus block. ABLd: ablation catheter.

Fig. 3 Activation times around the tricuspid annulus (TVA). A: flutter cycle length (FCL) is the activation time around the TVA. B: SD1: a shorter activation time between the lateral side of the cavotricuspid isthmus (CTI-L, pacing site) and line of conduction block (gray hatched). SD2: a longer activation time between the pacing site and line of block when the impulse turns anteriorly around the TVA. FCL=SD1+SD2.
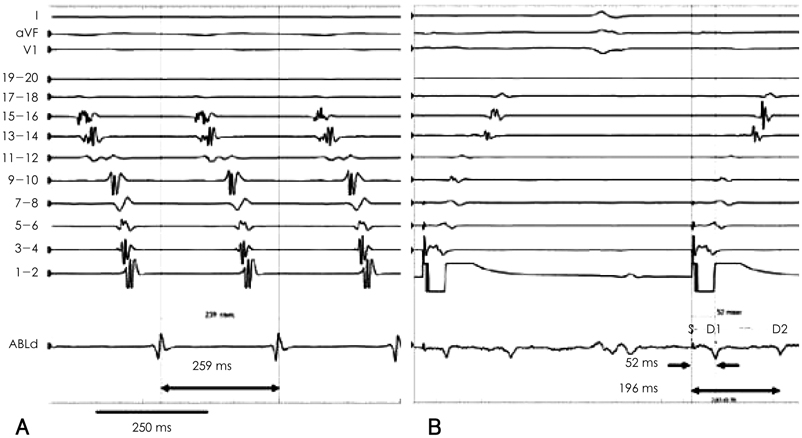
Fig. 4 Comparison between the flutter cycle length and the SDSUM. A: flutter cycle length (FCL) is 259 msec. B: conduction time taken from the stimulus (S) to the first potential (D1) of the split electrograms from ABLd, which corresponded to the counterclockwise distance from the lateral side of the cavotricuspid isthmus (CTI-L) to the ablation line in the isthmus, is 52 msec. Time from S to the second potential (D2), which corresponds to the clockwise conduction time from the CTI-L to the ablation line, when complete conduction block is achieved, is 196 msec. SDSUM is 248 ms (SD1+SD2 is nearly 95% of FCL). SDSUM: SD1+SD2, ABLd: ablation catheter.

Fig. 5 Comparison of SDSUMs (SD1+SD2) to the mean flutter cycle length (FCL). All measured data are standardized proportionally to the mean value of the FCL (224 ms). The upper 50 dots (closed circles) show SD1+SD2s during complete isthmus block and the lower 40 dots (open circle) show that of traversing the ablation line just before the block. The upper and lower dots are a one to one match, except for the absence of some of the lower dots. Line 202 means 90% of the mean FCL.

Fig. 6 Conduction delay as the pacing cycle length being shorter. A: Recording during continuous pacing after making a complete line of conduction block in the cavotricuspid isthmus at a cycle length of 600 msec results in an usual pacing cycle length during flutter ablation, in which SD2 was 169 msec. B: SD2 becomes longer in reverse proportion as the pacing cycle becomes shorter due to a conduction delay. When the pacing cycle length reaches the flutter cycle length, as in B, split electrograms become smaller and are frequently indistinguishable. Fortunately, split electrograms become distinguishable in this case after increasing the local gain of the ABLd recording. ABLd: ablation catheter.
Reference
-
1. Tada H, Oral H, Sticherling C, et al. Double potentials along the ablation line as a guide to radiofrequency ablation of typical atrial flutter. J Am Coll Cardiol. 2001. 38:750–755.2. Shah D, Haissaguerre M, Takahashi A, Jais P, Hocini M, Clementy J. Differential pacing for distinguishing block from persistent conduction through an ablation line. Circulation. 2000. 102:1517–1522.3. Oral H, Sticherling C, Tada H, et al. Role of transisthmus conduction intervals in predicting bidirectional block after ablation of typical atrial flutter. J Cardiovasc Electrophysiol. 2001. 12:169–174.4. Matsushita T, Chun S, Liem LB, Friday KJ, Sung RJ. Unidirectional conduction block at cavotricuspid isthmus created by radiofrequency catheter ablation in patients with typical atrial flutter. J Cardiovasc Electrophysiol. 2002. 13:1098–1102.5. Cosío FG, Awamleh P, Pastor A, Núñez A. Determining inferior vena cava-tricuspid isthmus block after typical atrial flutter ablation. Heart Rhythm. 2005. 2:328–332.6. Kim JJ, Kim YH, Chung SS, et al. Radiofrequency catheter ablation in patients with atrial flutter. Korean Circ J. 1996. 26:605–613.7. Saoudi N, Ricard P, Rinaldi JP, Yaïci K, Darmon JP, Anselme F. Methods to determine bidirectional block of the cavotricuspid isthmus in radiofrequency ablation of typical atrial flutter. J Cardiovasc Electrophysiol. 2005. 16:801–803.8. Mangat I, Tschopp DR Jr, Yang Y, Cheng J, Keung EC, Scheinman MM. Optimizing the detection of bidirectional block across the flutter isthmus for patients with typical isthmus-dependent atrial flutter. Am J Cardiol. 2003. 91:559–564.9. Deisenhofer I, Estner H, Zrenner B, et al. Left atrial tachycardia after circumferential pulmonary vein ablation for atrial fibrillation: incidence, electrophysiological characteristics, and results of radiofrequency ablation. Europace. 2006. 8:573–582.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Atrial Flutter
- Atrial Flutter Conversion in Infants and Children Using Transesophageal Atrial Pacing
- Radiofrequency Catheter Ablation in Patients with Atrial Flutter
- Transesophageal Atrial Pacing in Atrial Flutter
- Transient Conduction Block in Vasculitic Neuropathy Caused by Churg-strauss Syndrome: Transient Conduction Block in Vasculitic Neuropathy
