The Incidence and Pattern of Coronary Artery Anomalies in the North-West of Iran: A Coronary Arteriographic Study
- Affiliations
-
- 1Department of Cardiology, Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran. bahram.sohrabi@ymail.com
- KMID: 2224975
- DOI: http://doi.org/10.4070/kcj.2012.42.11.753
Abstract
- BACKGROUND AND OBJECTIVES
Coronary artery anomalies are found in approximately 1% of patients undergoing diagnostic coronary angiography (CAG). Angiographic recognition of these vessels is important because of their clinical significance and importance in patients undergoing coronary angioplasty or cardiac surgery. There are fairly enough reports concerning the incidence of coronary anomalies in different geographic areas, but this is the first study among the Iranian population.
SUBJECTS AND METHODS
We reviewed the database of the Catheterization Laboratory of Imam Reza and Shahid Madani Hospitals, Tabriz University of Medical Sciences, Iran. Our inquiry included all patients who referred for CAG from other hospitals, between February 2007 and April 2009. Patients with congenital heart diseases, high "take off" of coronary arteries and separate origin of the conus artery from the right coronary sinus (RCS) were excluded. In total, 6065 films were reviewed.
RESULTS
Seventy nine (1.30%) patients were found to have coronary anomalies. Seventy five (1.24%) patients had anomalies of origin and distribution, while four (0.06%) had coronary artery fistulae. Most common anomaly was separate ostia of the left anterior descending artery and left circumflex artery, which was found in 42 patients (53.16%) with angiographic incidence of 0.69%. The next most common anomalies were anomalous circumflex artery from RCS/right coronary artery (RCA) {n=17 (21.51%)}, and anomalous RCA arising from left coronary sinus {n=6 (7.59%)}.
CONCLUSION
In general, the incidence and pattern of coronary anomalies in our study was similar to earlier reports from different parts of the world.
Keyword
MeSH Terms
Figure
-

Fig. 1 Seperated LAD & LCX. Separate origins of LAD and LCX from the left coronary sinus. LAD: left anterior descending artery, LCX: left circumflex artery.
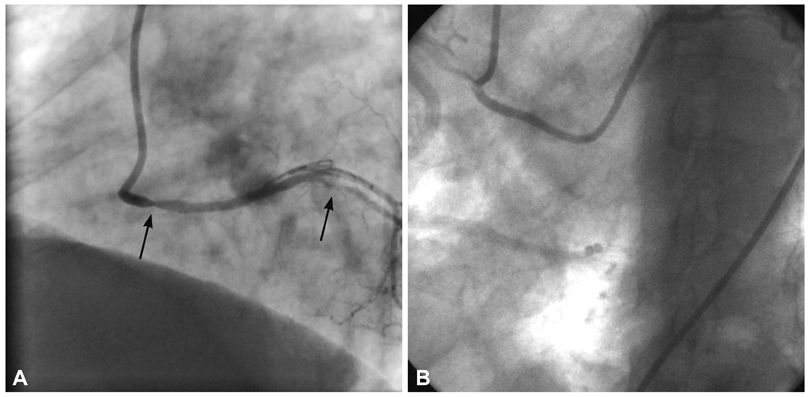
Fig. 2 Anomalous circumflex artery from the right coronary sinus (RCS)/right coronary artery. A: in one patient, left circumflex artery originates from right coronary sinus with significant coronary artery disease (arrow=lesion). B: another patient also had separate origins of conus artery and concomitant severe aortic regurgitation.
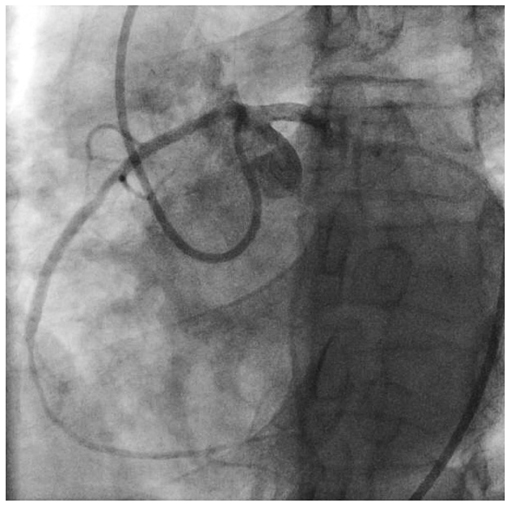
Fig. 3 RCA arising from LCS. RCA is originating from an orifice located anterior to LMCA ostium in the LCS and had interarterial course before reaching the right atrioventricular groove. RCA: right coronary artery, LCS: left coronary sinus, MLCA: left main coronary artery.
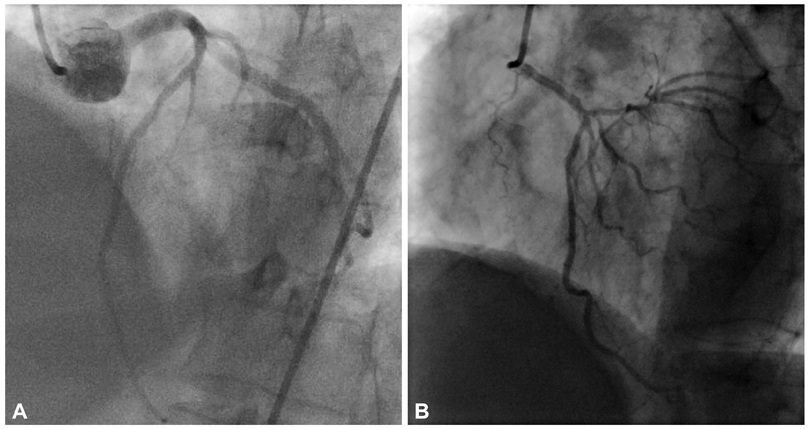
Fig. 4 LMCA arising from right coronary sinus. A: in this patient LMCA courses between aorta and pulmonary artery. B: a patient with anomalous LMCA with septal course. LMCA: left main coronary artery.
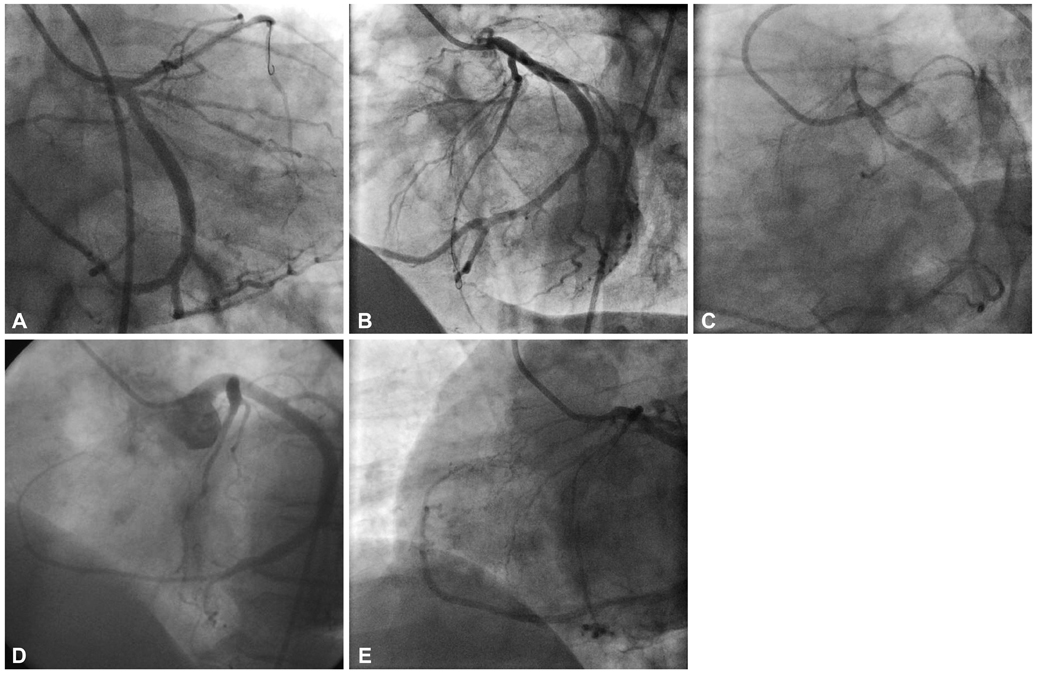
Fig. 5 Single coronary artery. Type I single coronary artery: the territory of right coronary artery is supplied by the continuation of left circumflex artery artery. A and B are different views of one patient and C, D and E are different views of another patient.
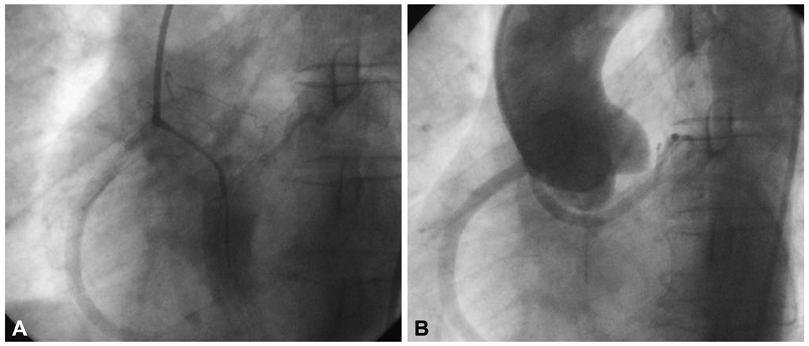
Fig. 6 Separated 3 coronary arteries. All 3 coronary arteries arising from right coronary sinus with separate osita. Distribution is normal. A: left anterior descending artery is diminutive and does not reach the apex and has septal course of its proximal part. B: circumflex artery originates from separate ostia and courses behind the aorta.

Fig. 7 Anomalous LCA from pulmonary artery. LCA is arising from pulmonary artery and was filing retrogradely via RCA. Both coronary arteries are enlarged, especially RCA. LCA: Left coronary artery, RCA: right coronary artery.
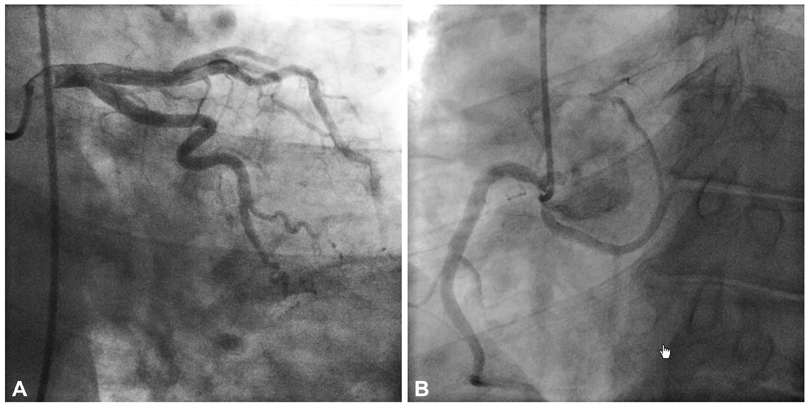
Fig. 8 Divided left circumflex artery. A: large obtuse marginalis, arising from left coronary artery. B: Aberrant circumflex artery from right coronary sinus.
Reference
-
1. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990. 21:28–40.2. Cieslinski G, Rapprich B, Kober G. Coronary anomalies: incidence and importance. Clin Cardiol. 1993. 16:711–715.3. Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, A not-so-minor congenital anomaly. Circulation. 1974. 50:780–787.4. Chaitman BR, Lespérance J, Saltiel J, Bourassa MG. Clinical, angiographic, and hemodynamic findings in patients with anomalous origin of the coronary arteries. Circulation. 1976. 53:122–131.5. Kragel AH, Roberts WC. Anomalous origin of either the right or left main coronary artery from the aorta with subsequent coursing between aorta and pulmonary trunk: analysis of 32 necropsy cases. Am J Cardiol. 1988. 62(10 Pt 1):771–777.6. Lee J, Choe YH, Kim HJ, Park JE. Magnetic resonance imaging demonstration of anomalous origin of the right coronary artery from the left coronary sinus associated with acute myocardial infarction. J Comput Assist Tomogr. 2003. 27:289–291.7. Aydinlar A, Ciçek D, Sentürk T, et al. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study in Western Turkey. Int Heart J. 2005. 46:97–103.8. Barriales Villa R, Morís C, López Muñiz A, et al. [Adult congenital anomalies of the coronary arteries described over 31 years of angiographic studies in the Asturias Principality: main angiographic and clinical characteristics]. Rev Esp Cardiol. 2001. 54:269–281.9. Harikrishnan S, Jacob SP, Tharakan J, et al. Congenital coronary anomalies of origin and distribution in adults: a coronary arteriographic study. Indian Heart J. 2002. 54:271–275.10. Kurjia HZ, Chaudhry MS, Olson TR. Coronary artery variation in a native Iraqi population. Cathet Cardiovasc Diagn. 1986. 12:386–390.11. Topaz O, DiSciascio G, Cowley MJ, et al. Absent left main coronary artery: angiographic findings in 83 patients with separate ostia of the left anterior descending and circumflex arteries at the left aortic sinus. Am Heart J. 1991. 122:447–452.12. Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary: arteriographic study. Int J Cardiol. 2000. 74:39–46.13. Ouali S, Neffeti E, Sendid K, Elghoul K, Remedi F, Boughzela E. Congenital anomalous aortic origins of the coronary arteries in adults: a Tunisian coronary arteriography study. Arch Cardiovasc Dis. 2009. 102:201–208.14. Correia E, Ferreira P, Rodrigues B, et al. Prevalence of anomalous origin of coronary arteries: a retrospective study in a Portuguese population. Rev Port Cardiol. 2010. 29:221–229.15. Göl MK, Ozatik MA, Kunt A, et al. Coronary artery anomalies in adult patients. Med Sci Monit. 2002. 8:CR636–CR641.16. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979. 130:39–47.17. Chan CN, Berland J, Cribier A, Letac B. Angioplasty of the right coronary artery with origin of all three coronary arteries from a single ostium in the right sinus of Valsalva. Am Heart J. 1993. 126:985–987.18. Lawton J, McGrath J, Jones JS, Dehmer GJ. Treatment of coronary artery disease in an anomalous coronary artery by placement of an intracoronary stent. Cathet Cardiovasc Diagn. 1997. 41:185–188.19. Hsu LA, Chu PH, Ko YS, Ko YL, Chiang CW. Transluminal coronary angioplasty and stenting in a patient with single coronary artery and acute myocardial infarction. Changgeng Yi Xue Za Zhi. 1997. 20:299–303.20. Gambhir DS, Singh S, Bharadwaj S, Arora R. Rotablation and elective stenting of stenosis in the left anterior descending coronary artery arising from an anomalous single coronary artery. Indian Heart J. 2000. 52:459–460.21. Stefenelli T, Wutte M, Madl C, Weissel M. Emergency angioplasty and stent deployment for acute occlusion of an anomalous single coronary artery (all three coronary arteries from one ostium in the right sinus of Valsalva). Wien Klin Wochenschr. 2001. 113:138–140.22. Ohta H, Sumiyoshi M, Suwa S, et al. Primary coronary angioplasty with stenting for acute coronary syndrome in patients with isolated single coronary artery: a report of 2 cases. Jpn Heart J. 2003. 44:759–765.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Coronary Artery Dissection and Woven Coronary Artery: Three Cases and a Review of the Literature
- A Case of Right Coronary Artery Originating from Distal Left Circumflex (Single Coronary Artery)
- Coronary Artery Anomaly, What Radiologist Should Know?
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
- Anomalous Origin of the Right Coronary Artery from the Left Anterior Descending Artery: An Extremely Rare Variety of Single Coronary Artery
