Right Coronary Artery to Left Ventricular Fistula Associated with Infective Endocarditis of the Mitral Valve
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine and Sejong Medical Research Institute, Sejong General Hospital, Bucheon, Korea. yoorimbin@sejongh.co.kr
- KMID: 2224954
- DOI: http://doi.org/10.4070/kcj.2013.43.4.281
Abstract
- A 27-year-old man with bacterial endocarditis of the mitral valve and embolic episodes was bound to have a large right coronary artery fistula communicating with the left ventricle, immediately inferior to the posterior mitral annulus. The perforation of the posterior leaflet and coronary arteriovenous fistula was identified using two-dimensional Doppler echocardiography. The diagnosis was confirmed by coronary angiography, and the patient underwent a successful operation.
MeSH Terms
Figure
-
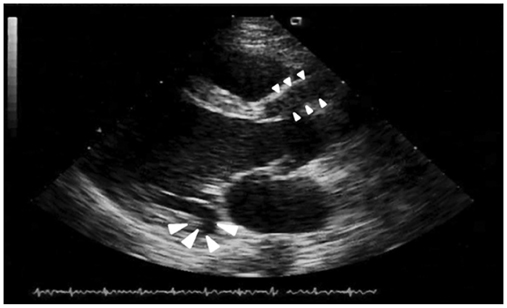
Fig. 1 Parasternal long axis echocardiogram showing the echo free space beneath the posterior mitral annulus (large arrowheads) and aneurysmal dilation of the proximal right coronary artery (small arrowheads).

Fig. 2 A: parasternal short axis echocardiogram showing the site of drainage of the fistulous tract into the left ventricle (arrowheads). B: parasternal short axis echocardiogram with color Doppler showing blood flow from the fistula into the left ventricle (arrowhead).
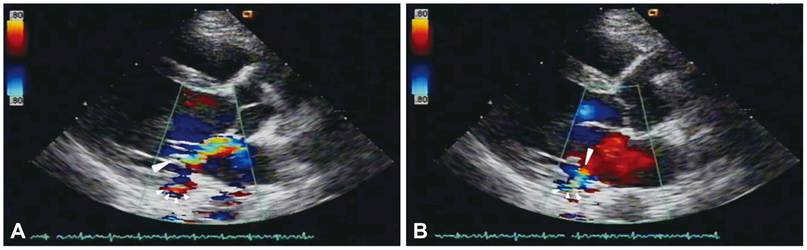
Fig. 3 A: parasternal long axis echocardiogram with color flow Doppler during isovolumetric ventricular contraction showing high velocity turbulent flow striking the posterior mitral leaflet (large arrowhead) near the drainage site of coronary arteriovenous fistula (small arrowheads). B: parasternal long axis echocardiogram with color flow Doppler during diastole showing laminar flow through the perforation of the posterior mitral leaflet (large arrowhead).
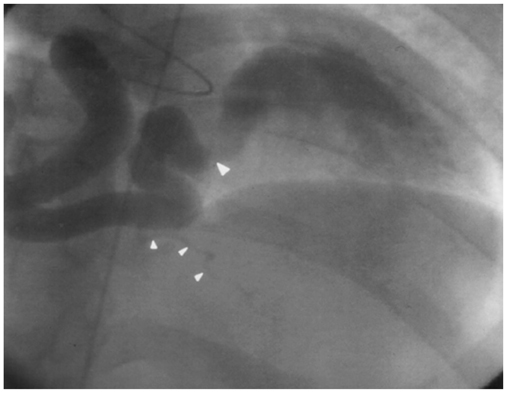
Fig. 4 Anterioposterior cranial view of the coronary angiogram showing a dilated and tortuous right coronary arteriovenous fistula drainage into the left ventricle (large arrowhead). One normal looking posterior descending artery is observed (small arrowheads).
Reference
-
1. Liberthson RR, Sagar K, Berkoben JP, Weintraub RM, Levine FH. Congenital coronary arteriovenous fistula. Report of 13 patients, review of the literature and delineation of management. Circulation. 1979. 59:849–854.2. Rittenhouse EA, Doty DB, Ehrenhaft JL. Congenital coronary arterycardiac chamber fistula. Review of operative management. Ann Thorac Surg. 1975. 20:468–485.3. Ong ML. Endocarditis of the tricuspid valve associated with congenital coronary arteriovenous fistula. Br Heart J. 1993. 70:276–277. discussion 277-8.4. Lee CW, Sung SH, Yu WC. Coronary artery fistula with a huge aneurysm formation presenting as heart failure. Korean Circ J. 2012. 42:69–70.5. Edwards JE. Mitral insufficiency secondary to aortic valvular bacterial endocarditis. Circulation. 1972. 46:623–626.6. Miyatake K, Okamoto M, Kinoshita N, Fusejima K, Sakakibara H, Nimura Y. Doppler echocardiographic features of coronary arteriovenous fistula. Complementary roles of cross sectional echocardiography and the Doppler technique. Br Heart J. 1984. 51:508–518.7. Kimball TR, Daniels SR, Meyer RA, Knilans TK, Plowden JS, Schwartz DC. Color flow mapping in the diagnosis of coronary artery fistula in the neonate: benefits and limitations. Am Heart J. 1989. 117:968–971.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Communication between the Pulmonary Artery and Vieussens’ Arterial Ring Causing Infective Endocarditis
- Right Coronary Artery to Left Ventricular Fistula with a Giant Right Coronary Artery Aneurysm: A case report
- A Case of Infective Endocarditis Complicated with Multiple Myocotic Aneurysm and Mitral Valve Perforation
- A Case of Congenital Coronary Arteriovenous Fistula Presented as Congestive Heart Failure and Aortic Valve Infective Endocarditis
- Infective Left Atrial Dissecting Flap after Cardiac Surgery
