A Two Cases of Primary Tuberculosis at the Nasopharynx
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. siamkhy@gmail.com
- KMID: 2223210
- DOI: http://doi.org/10.18787/jr.2015.22.2.123
Abstract
- Upper airway tuberculosis usually develops as a secondary infection from pulmonary tuberculosis, and primary upper airway tuberculosis, especially in nasopharynx, is a rare disease. The appropriate treatment for nasopharyngeal tuberculosis has been difficult because of complicated initial diagnosis and suspicion. Physicians should consider various granulomatous diseases in differential diagnosis. However, upper airway tuberculosis can be highly contagious, like pulmonary tuberculosis; therefore, early diagnosis and proper management are important. We recently experienced the successful early diagnosis and treatment of two cases of nasopharyngeal tuberculosis and report these cases with a review of the literature.
Keyword
MeSH Terms
Figure
-

Fig. 1. Initial 90° endoscopic finding demonstrated necrotic tissue (black arrow) with purulent discharge on left lateral and posterior wall of nasopharynx (A), and right anterior moderate tympanic menbrane perforation with otorrhea (B). Follow-up examinations which were performed 1month after surgery showed completely healed nasopharynx (C), and decreased otorrhea of right ear (D).

Fig. 2. Preoperative computed tomography revealed poorly enhancing central soft tissue with peripheral rim enhancing lesion (white arrow) at the left lateral and posterior wall of nasopharynx.
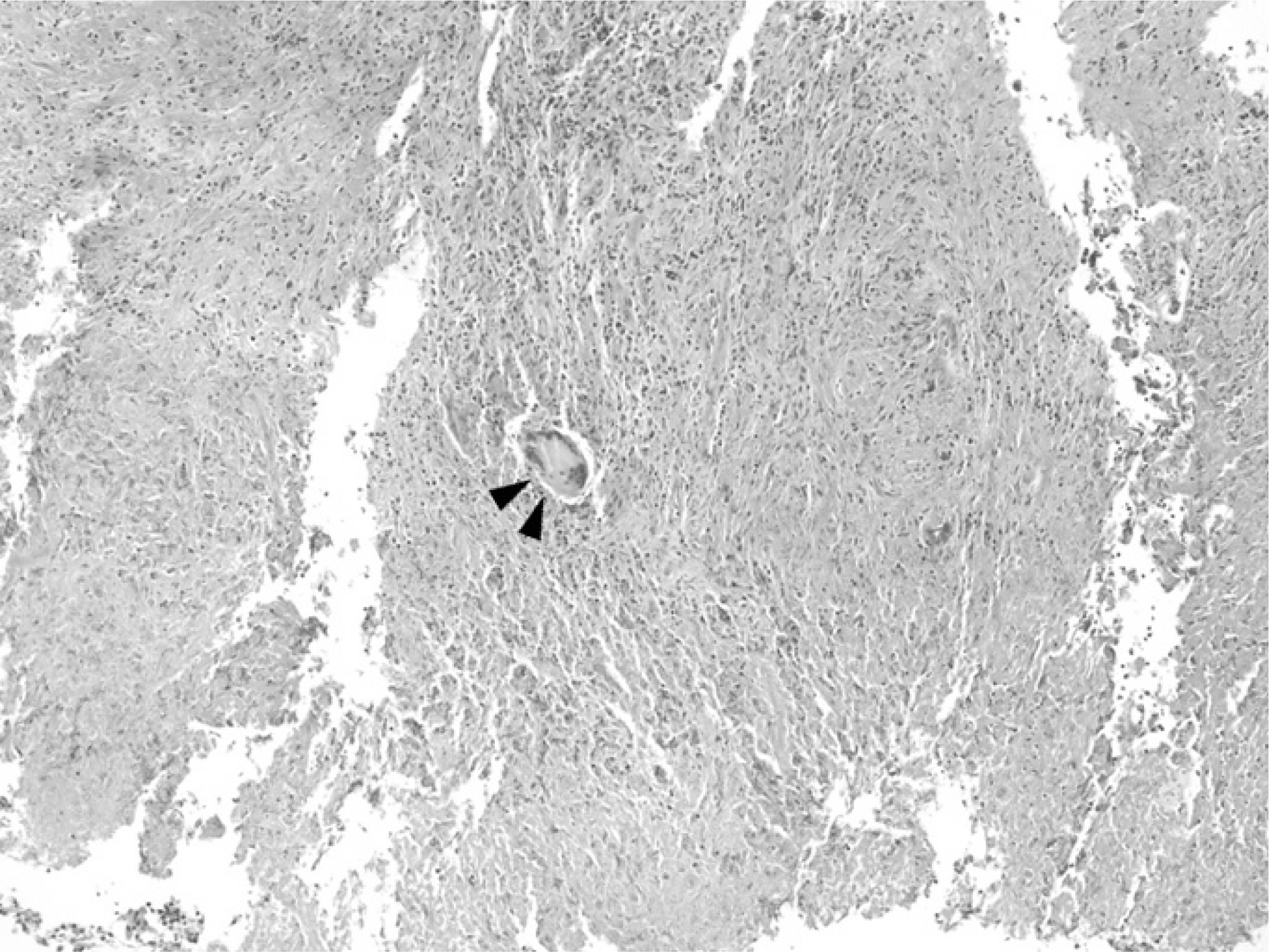
Fig. 3. Nasopharyngeal tissue shows the caseous necrosis (black arrow head) and granulomatous inflammation with inflammatory cell infiltration in this photomicrograph of surgical biopsy (H&E, ×100).

Fi. 4. Initial 90o (A) and 30o (B) endoscopic finding demonstrated necrotic tissue (black arrow) and mucosal swelling with purulent discharge on nasopharynx wall entirely, Follow-up examinations which were performed 15 days after surgery showed partially improved of nasopharynx necrotic mucosa (C), and 1 month after surgery showed completely healed nasopharynx (D).

Fig. 5. Preoperative computed tomography showed increased enhancement and mild wall thickening of nasopharyngeal mucosa.
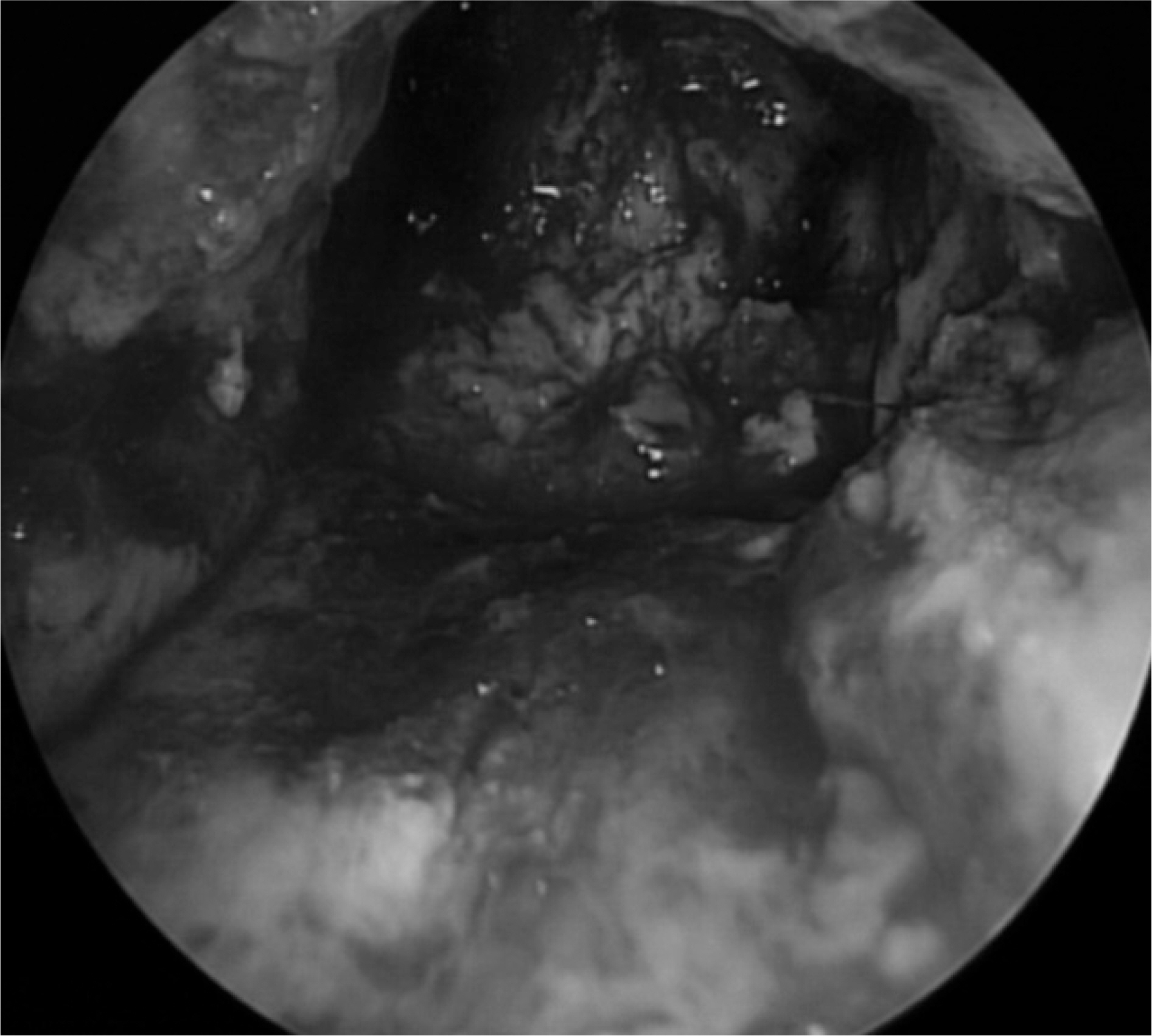
Fig. 6. Endoscopic debridement of nasopharynx.
Cited by 2 articles
-
A Case of Primary Tuberculosis of the Lacrimal Sac Presenting as Epiphora
Sang Yun Lee, Sangwook Park, Jong-Sil Lee, Yung Jin Jeon
Korean J Otorhinolaryngol-Head Neck Surg. 2021;64(3):202-206. doi: 10.3342/kjorl-hns.2020.00213.Two Cases of Primary Nasopharyngeal Tuberculosis
Ha Na Lee, Seon Min Jung, Seok Hyun Cho, Jin Hyeok Jeong
J Rhinol. 2022;29(3):167-171. doi: 10.18787/jr.2022.00409.
Reference
-
References
1). WHO. Global Report. Global tuberculosis control: surveillance, planning, financing. Geneva, Switzerland: WHO;2005.2). Kim HJ. Current Status of Tuberculosis in Korea. Korean Journal of Medicine. 2012; 82:257.
Article3). Srirompotong S, Yimtae K, Jintakanon D. Nasopharyngeal tuberculosis: manifestations between 1991 and 2000. Otolaryngology–head and neck surgery: official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2004; 131:762–4.
Article4). Kawamura I, Kudo T, Tsukahara M, Kurai H. Infection control for extrapulmonary tuberculosis at a tertiary care cancer center. American Journal of Infection Control. 2014; 42:1133–5.
Article5). Kim TH, Hong JW, Lee JH, Kim MG. A Case of Nasopharyngeal Tuberculosis Resulting in Tuberculous Otitis Media. Korean Journal of Otolaryngology-Head and Neck Surgery. 2009; 52:245.
Article6). Waldron J, Van Hasselt CA, Skinner DW, Arnold M. Tuberculosis of the nasopharynx: clinicopathological features. Clinical otolaryngology and allied sciences. 1992; 17:57–9.
Article7). August M, Dodson TB, Nastri A, Chuang SK. Nasopharyngeal carcinoma: clinical assessment and review of 176 cases. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics. 2001; 91:205–14.
Article8). Sharma SK, Mohan A. Extrapulmonary tuberculosis. The Indian Journal of Medical Research. 2004; 120:316–53.
Article9). Koktener A. Nasopharyngeal tuberculosis. European journal of radiology. 2001; 39:186–7.
Article10). Chan AB, Ma TK, Yu BK, King AD, Ho FN, Tse GM. Nasopharyngeal granulomatous inflammation and tuberculosis complicating undifferentiated carcinoma. Otolaryngology–head and neck surgery: Official Journal of American Academy of Otolaryngolo-gy-Head and Neck Surgery. 2004; 130:125–30.
Article11). Cai PQ, Li YZ, Zeng RF, Xu JH, Xie CM, Wu YP, et al. Nasopharyngeal tuberculosis: CT and MRI findings in thirty-six patients. European Journal of Radiology. 2013; 82:e448–54.
Article12). Starke JR. Interferon-gamma Release Assays for Diagnosis of Tuberculosis Infection and Disease in Children. Pediatrics. 2014.13). Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in healthcare settings, 2005. MMWR Recomm Rep. 2005; 54:1–141.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Nasopharyngeal Tuberculosis
- Two Cases of Primary Nasopharyngeal Tuberculosis
- A case of primary nasopharyngeal tuberculosis with cervical lymphadenitis of immigrant woman from Vietnam
- Six Cases of Nasal Cavity and Nasopharyngeal Tuberculosis
- A Case of Nasopharyngeal Tuberculosis with Retropharyngeal Abscess
