J Korean Ophthalmol Soc.
2013 Jan;54(1):180-183. 10.3341/jkos.2013.54.1.180.
Orbital Emphysema Causing Eye Movement Restriction Without Orbital Fractures Due to Compressed Air Injury
- Affiliations
-
- 1Department of Ophthalmology, Gachon University Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea. cmj@gilhospital.com
- 2Osan Bright Eye Clinic, Osan, Korea.
- KMID: 2216470
- DOI: http://doi.org/10.3341/jkos.2013.54.1.180
Abstract
- PURPOSE
The authors experienced a case of orbital emphysema causing eye movement disorder following conjunctival tear without any orbital wall fractures after exposure to compressed air.
CASE SUMMARY
A 28-year-old man's left periorbital area was injured while working with compressed air. There was marked lid swelling on the left side with palpable crepitus. The patient had an exotropia and hypertropia of the left eye. In addition, the extraocular movement of the left eye was restricted on upgaze without nausea and vomiting. On slit-lamp examination, conjunctival partial laceration and subconjunctival air bubbles adjacent to the conjunctival laceration could be seen. Orbital computed tomography showed air in the periorbital and retrobulbar region of the left eye and no evidence of orbital fracture. On examination 4 days after the primary repair of the conjunctival laceration, the patient completely recovered without any complication.
CONCLUSIONS
Orbital emphysema following a conjunctival laceration caused by compressed air without any orbital wall fractures can cause restriction of eye movement.
MeSH Terms
Figure
-
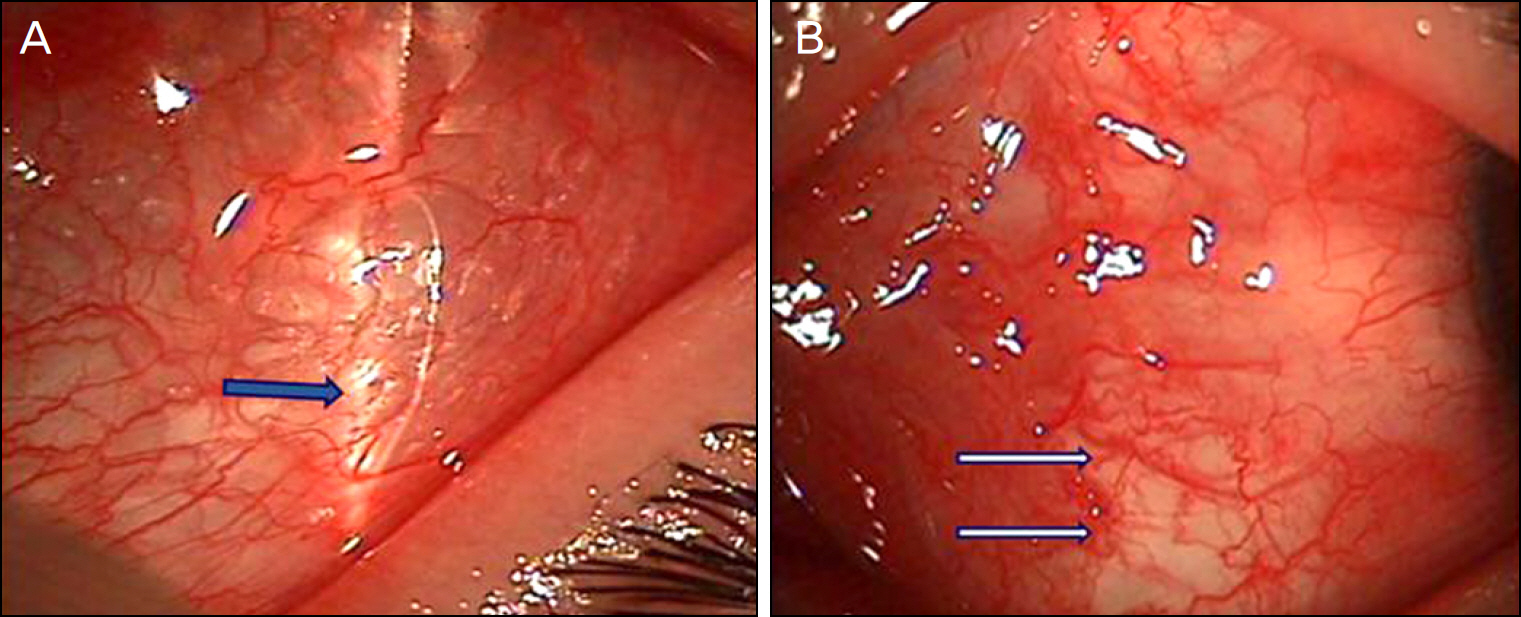
Figure 1. On slitlamp examination, subconjunctival air bubbles (A, black arrow) and conjunctival partial laceration (B, white arrows) could be seen.

Figure 2. He had an exotropia and hypertropia of the left eye (A). And the extraocular movement of left eye was restricted on upgaze (B).
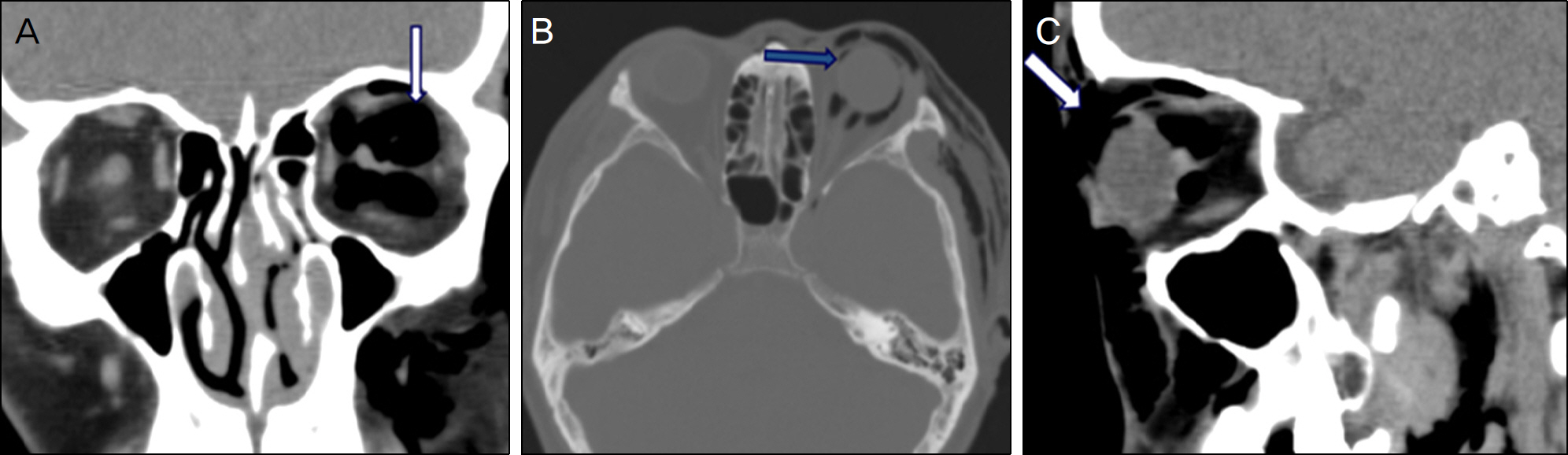
Figure 3. Orbital CT scan shows air in the retrobulbar (A, white arrow), subconjunctival (B, black arrow), and subcutaneous (C, thick white arrow) area. Superior rectus muscle is downwardly positioned. There aren't any orbital wall fractures.
Reference
-
References
1. Caesar R, Gajus M, Davies R. Compressed air injury of the orbit in the absence of external trauma. Eye (Lond). 2003; 17:661–2.
Article2. Li T, Mafee MF, Edward DP. Bilateral orbital emphysema from compressed air injury. Am J Ophthalmol. 1999; 128:103–4.
Article3. Yuksel M, Yuksel KZ, Ozdemir G, Ugur T. Bilateral orbital abdominal and pneumocephalus as a result of accidental compressed air exposure. Emerg Radiol. 2007; 13:195–8.4. Stroh EM, Finger PT. Traumatic transconjunctival orbital emphysema. Br J Ophthalmol. 1990; 74:380–1.
Article5. Lubniewski AJ, Feibel RM. Traumatic air blast injury with abdominal, bilateral orbital, and mediastinal air. Ophthalmic Surg. 1989; 20:677–9.6. Mathew S, Vasu U, Francis F, Nazareth C. Transconjunctival abdominal emphysema caused by compressed air injury: a case report. Indian J Ophthalmol. 2008; 56:247–9.7. Biger Y, Abulafia C. Subconjunctival emphysema due to trauma by compressed air tube. Br J Ophthalmol. 1986; 70:227–8.
Article8. Gross JG, Doxanas MT. Traumatic optic atrophy caused by abdominal air. Ann Ophthalmol. 1987; 19:69–70. 74.9. Linberg JV. Orbital emphysema complicated by acute central abdominall artery occlusion: case report and treatment. Ann Ophthalmol. 1982; 14:747–9.10. Dobler AA, Nathenson AL, Cameron JD, et al. A case of orbital emphysema as an ocular emergency. Retina. 1993; 13:166–8.
Article11. Hunts JH, Patrinely JR, Holds JB, Anderson RL. Orbital emphysema. Staging and acute management. Ophthalmology. 1994; 101:960–6.12. Burt B, Jamieson M, Sloan B. Medial wall fracture-induced pneumo-orbita mimicking inferior rectus entrapment. Am J Emerg Med. 2010; 28:119. e1–3.13. Roccia F, Griffa A, Nasi A, Baragiotta N. Severe subcutaneous abdominal and pneumomediastinum associated with minor max-illofacial trauma. J Craniofac Surg. 2003; 14:880–3.14. Papadimitriou P, Ntomouchtsis A, Antoniades K. Delayed abdominal ocular emphysema: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:e18–20.15. Silver HS, Fucci MJ, Flanagan JC, Lowry LD. Severe orbital abdominal as a complication of orbital fracture. Arch Otolaryngol Head Neck Surg. 1992; 118:845–8. discussion 882.16. Mohan B, Singh KP. Bilateral subcutaneous emphysema of the abdominals following nose blowing. J Laryngol Otol. 2001; 115:319–20.17. Gonzalez F, Cal V, Elhendi W. Orbital emphysema after sneezing. Ophthal Plast Reconstr Surg. 2005; 21:309–11.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Orbital Emphysema and Pneumocephalus Caused by Compressed Air Injury
- Clinical course of compressed air injury with pneumocephlaus and orbital emphysema: a case report
- Near-complete optic nerve transection by high-pressure air
- A Case of Orbital Emphysema after Nose Blowing
- Pneumocephalus due to Compressed Air Injury without Facial Bone Fracture
