Short-Term Outcome of Intravitreal Dexamethasone Implant for Macular Edema Secondary to Branch Retinal Vein Occlusion
- Affiliations
-
- 1Department of Ophthalmology, Kim's Eye Hospital, Konyang University College of Medicine, Seoul, Korea. kjh7997@daum.net
- KMID: 2216152
- DOI: http://doi.org/10.3341/jkos.2015.56.1.39
Abstract
- PURPOSE
To evaluate short-term outcomes of intavitreal dexamethasone implant in macular edema secondary to branch retinal vein occlusion (BRVO).
METHODS
A retrospective review of medical records was performed for 24 patients (24 eyes) who were diagnosed with macular edema secondary to BRVO. The best-corrected visual acuity (BCVA) and central foveal thickness (CFT) were measured before the injection and at 1 and 3 months after the injection. The values measured before and after the treatment were compared. In addition, the association between duration of symptoms and 3-month changes in BCVA was evaluated.
RESULTS
In 24 eyes, the logarithm of minimal angle of resolution BCVA before the injection and 1 and 3 months after the injection was 0.56 +/- 0.25, 0.42 +/- 0.26 and 0.45 +/- 0.27, respectively. The CFT was 550.2 +/- 116.5 microm, 270.3 +/- 101.5 microm, and 356.6 +/- 173.7 microm, respectively. When compared with the baseline values, the BCVA at 3 months was significantly improved (p = 0.018) and the CFT was significantly decreased (p < 0.001). There was a significant negative association between the duration of symptoms and 3-month changes in BCVA (p = 0.032, r = -0.375). Elevated intraocular pressure was observed in 3 eyes (12.5%).
CONCLUSIONS
Intravitreal dexamethasone implant was found effective in treating macular edema secondary to BRVO. However, rebound macular edema and deterioration in visual acuity after 1 month suggest further studies with longer follow-ups are necessary.
MeSH Terms
Figure
-
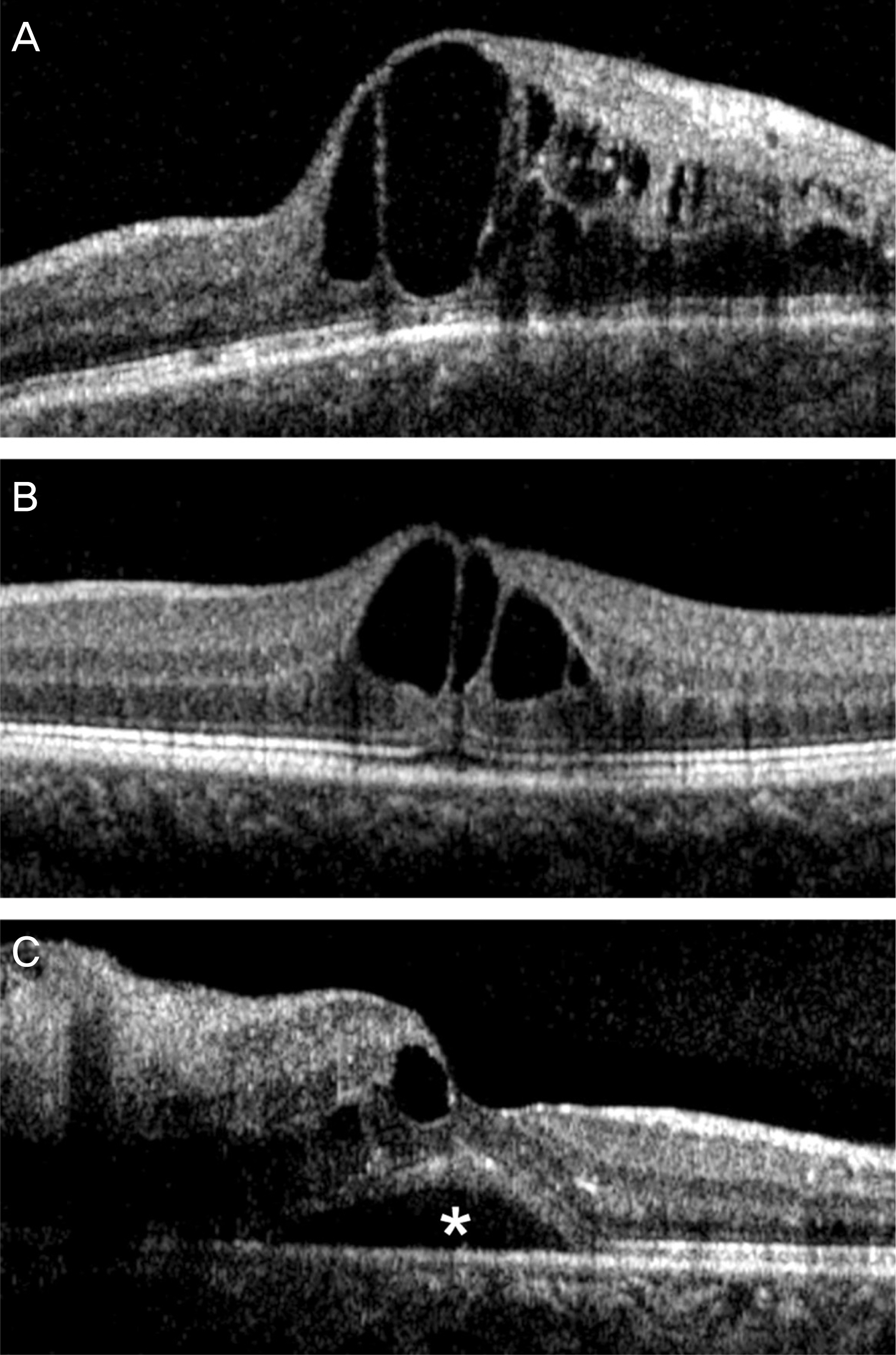
Figure 1. Optical coherence tomography based classification of macular edema in branch retinal vein occlusion, as recommended by Park and Rho.13 (A) Diffuse thickening of the entire retinal layer. (B) Focal thickening of the retina. (C) Macular edema with serous retinal detachment (asterisk).

Figure 2. Changes in logarithm of minimal angle of resolution (log MAR) best-corrected visual acuity (A, BCVA) and central foveal thickness (B) in eyes with macular edema secondary to retinal vein occlusion that were treated with intravitreal dexamethasone implant. Statistical analysis was performed using paired t-test and repeated measures analysis of variances with a Bonferroni’s correction.

Figure 3. Fundus photography (A, B) and optical coherence tomography (right column) images in an eye with branch retinal vein occlusion. (A) A fundus photography taken at diagnosis. (B) A fundus photography taken 3 days after intravitreal injection of dexamethasone implant. An arrow indicates intravitreal implant. Optical coherence tomography images showing macular microstructure at diagnosis (C), 1 month after intravitreal injection of bevacizumab (D), and 3 month after intravitreal injection of dexamethasone implant (E). The best-corrected visual acuity improved from 20/200 to 20/60 after injection of dexamethasone implant.
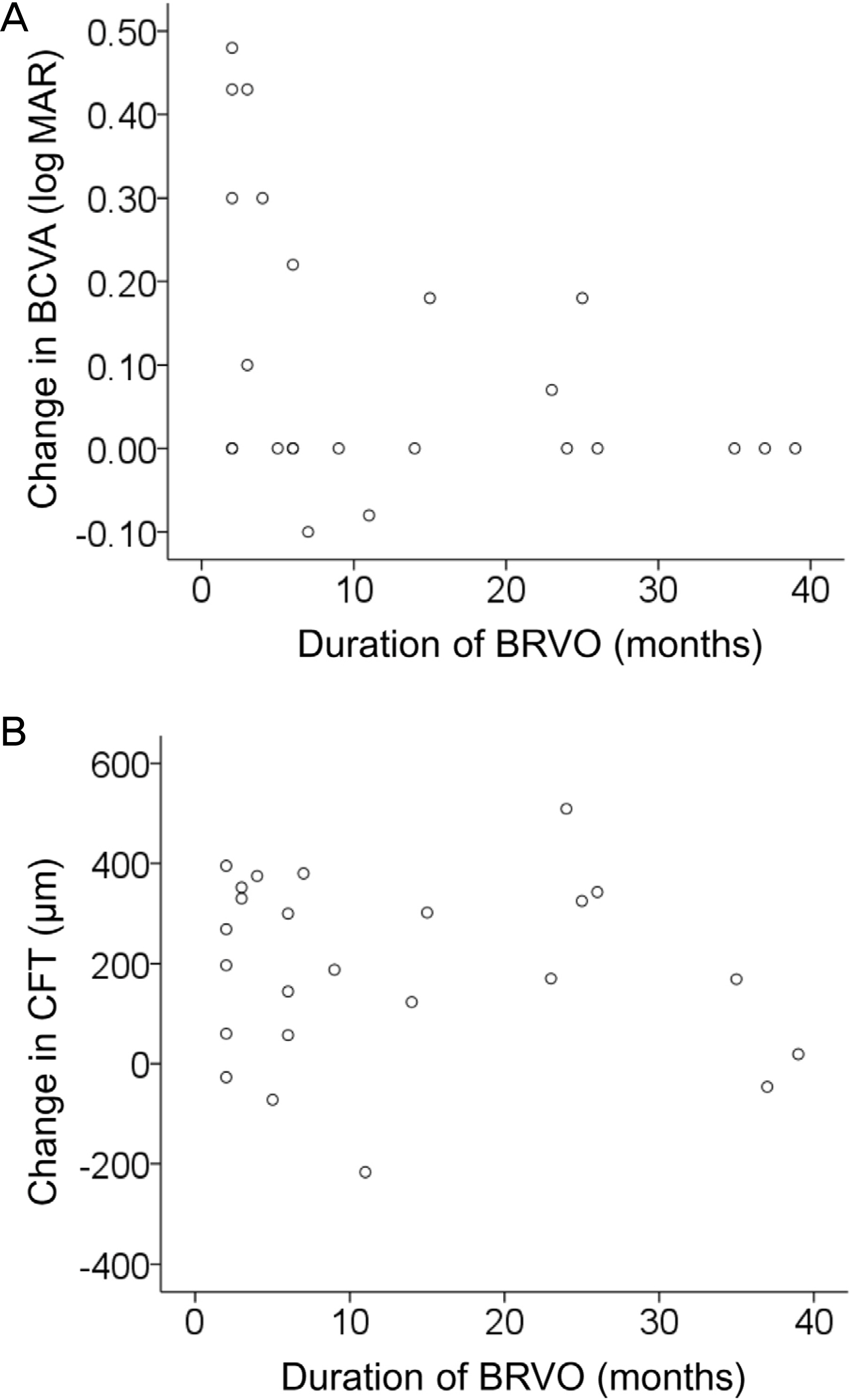
Figure 4. Changes in best-corrected visual acuity (BCVA, A) and central foveal thickness (CFT, B) before and one month after intravitreal injection of dexamethasone implant, according to the duration of branch retinal vein occlusion (BRVO). Positive values indicate improvement in BCVA or decrease in CFT, whereas negative values indicate deterioration in BCVA or increase in CFT. There was a significant negative association between the change in BCVA and the duration of BRVO (A, p = 0.032, r = -0.375), whereas the association between the change in CFT and the duration was not significant (B, p = 0.625). log MAR = logarithm of minimal angle of resolution.
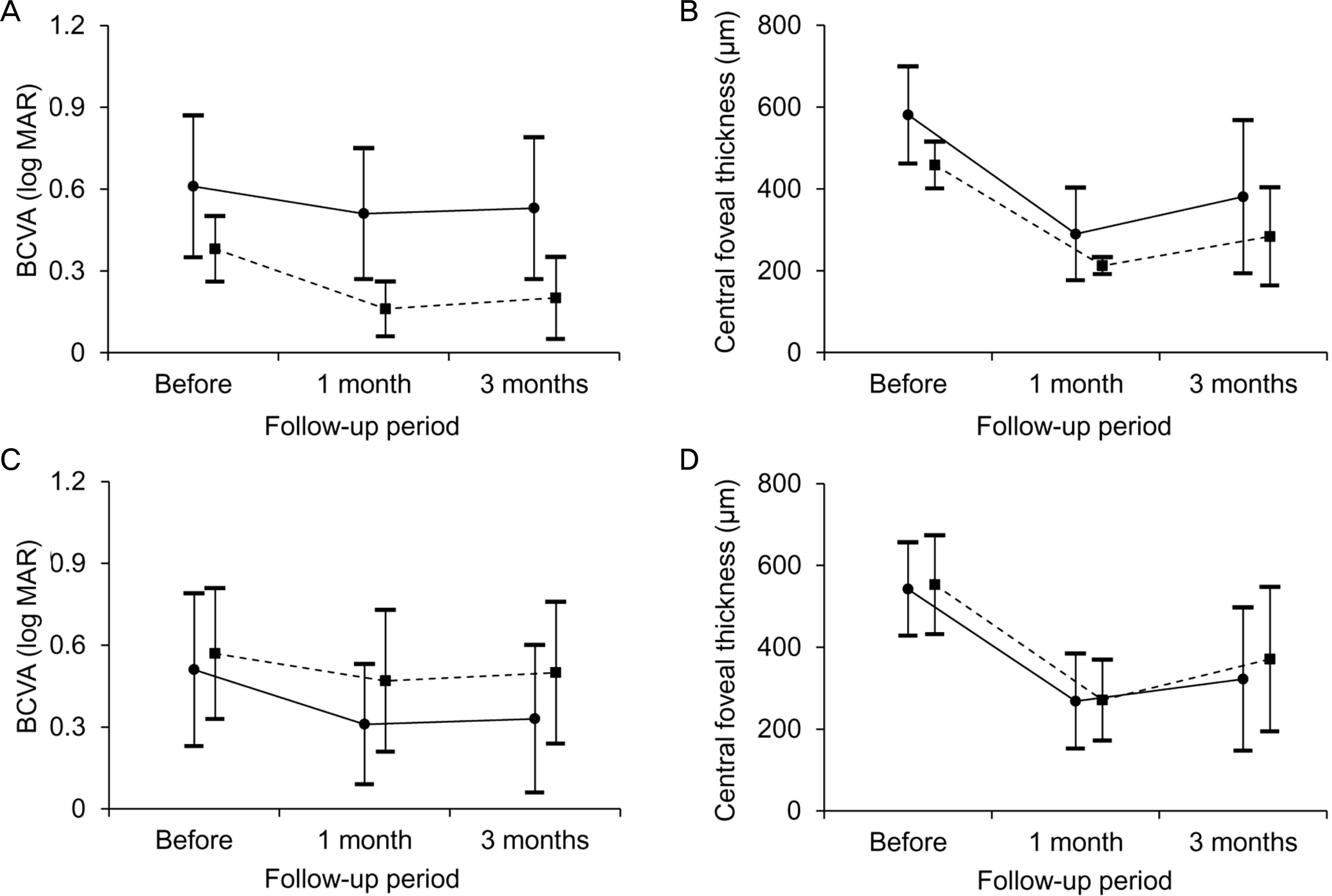
Figure 5. Changes in best-corrected visual acuity (BCVA) and central foveal thickness in eyes with macular edema secondary to branch retinal vein occlusion when divided into 2 groups, according to the characteristic of macular edema. (A, B) Closed circle (solid line, n = 18) indicates eyes with diffuse thickening of the entire retinal layer, whereas a closed square (dashed line, n = 6) indicates eyes with focal thickening of the retina. (C, D) Closed circle (solid line, n = 7) indicates eyes with serous retinal detach-ment, whereas a closed square (dashed line, n = 17) indicates eyes without serous retinal detachment.
Reference
-
References
1. Hayreh SS. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog Retin Eye Res. 2005; 24:493–519.
Article2. Rogers SL, McIntosh RL, Lim L. . Natural history of branch retinal vein occlusion: an evidence-based systematic review. Ophthalmology. 2010; 117:1094–101.e5.
Article3. McIntosh RL, Rogers SL, Lim L. . Natural history of central retinal vein occlusion: an evidence-based systematic review. Ophthalmology. 2010; 117:1113–23.e15.
Article4. Campochiaro PA, Hafiz G, Shah SM. . Ranibizumab for macular edema due to retinal vein occlusions: implication of VEGF as a critical stimulator. Mol Ther. 2008; 16:791–9.
Article5. Shin HY, Jee DH. The short-term efficacy of intravitreal ranibizu-mab for macular edema in central retinal vein occlusion. J Korean Ophthalmol Soc. 2011; 52:1048–54.
Article6. Lee YS, Kim MS, Yu SY, Kwak HW. Two-year results of intra-vitreal bevacizumab injection in retinal vein occlusion. J Korean Ophthalmol Soc. 2011; 52:1039–47.
Article7. Campochiaro PA, Brown DM, Awh CC. . Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve-month outcomes of a phase III study. Ophthalmology. 2011; 118:2041–9.
Article8. Brown DM, Campochiaro PA, Bhisitkul RB. . Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology. 2011; 118:1594–602.
Article9. Kuppermann BD, Blumenkranz MS, Haller JA. . Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007; 125:309–17.
Article10. Haller JA, Bandello F, Belfort R Jr. . Randomized, sham-con-trolled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010; 117:1134–46.e3.
Article11. Youn SM, Park SJ, Lee HY. . A case of dexamethasone intravitreal implant fragmentation during the injection procedure in central retinal vein occlusion. J Korean Ophthalmol Soc. 2013; 54:982–6.
Article12. Han HC, Bang JW, Yum JH. . A case of acute endophthalmitis following a dexamethasone intravitreal implant. J Korean Ophthalmol Soc. 2013; 54:1939–44.
Article13. Park KH, Rho IH. Short-term visual outcomes according to patterns of macular edema in retinal vein occlusion patients. J Korean Ophthalmol Soc. 2012; 53:1276–84.
Article14. Joshi L, Yaganti S, Gemenetzi M. . Dexamethasone implants in retinal vein occlusion: 12-month clinical effectiveness using repeat injections as-needed. Br J Ophthalmol. 2013; 97:1040–4.
Article15. Matonti F, Meyer F, Guigou S. . Ozurdex in the management of the macular edema following retinal vein occlusion in clinical practice. Acta Ophthalmol. 2013; 91:e584–6.
Article16. Sharareh B, Gallemore R, Taban M. . Recalcitrant macular edema after intravitreal bevacizumab is responsive to an intravitreal dexamethasone implant in retinal vein occlusion. Retina. 2013; 33:1227–31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Retinal Hemorrhage Following a Dexamethasone Intravitreal Implant
- A Comparison of Three Intravitreal Modalities of Branch Retinal Vein Occlusion Macular Edema
- Intravitreal Dexamethasone Implant for Macular Edema in Branch Retinal Vein Occlusion According to Previous Responses to Bevacizumab
- A Case of Dexamethasone Intravitreal Implant Fragmentation During the Injection Procedure in Central Retinal Vein Occlusion
- A Case of Acute Endophthalmitis Following a Dexamethasone Intravitreal Implant
