Analysis of Internal Optical Aberrations in Eyes with Different Types of Cataract
- Affiliations
-
- 1Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea. crisim@korea.ac.kr
- KMID: 2215703
- DOI: http://doi.org/10.3341/jkos.2015.56.4.532
Abstract
- PURPOSE
The present study investigates the patterns of internal optical aberrations in eyes with different types of cataract.
METHODS
Eighty eyes of 70 cataract patients were included in the present study. Internal optical aberrations were measured with a KR-1W wavefront aberrometer before cataract operation. Types of cataract were classified into three groups; cortical, nuclear and posterior subcapsular cataracts. The differences in the results of the wavefront data of 6-mm pupil diameter zones were compared among three groups. The Kruskal-Wallis test and Mann-Whitney U test were used for comparing data.
RESULTS
A total of 80 eyes consisting of 30 cortical cataracts, 30 nuclear cataracts and 20 posterior subcapsular cataracts were found. In the 6-mm pupil diameter zone, the average internal spherical aberrations by original value were 0.042 microm of cortical cataracts, -0.092 microm of nuclear cataracts and -0.109 microm of posterior subcapsular cataracts. The average internal spherical aberrations by absolute value were 0.122 microm of cortical cataracts, 0.533 microm of nuclear cataracts and 0.202 microm of posterior subcapsular cataracts. The internal spherical aberrations by original value were not statistically significantly different, but by absolute value were statistically significantly different (p = 0.003, Kruskal-Wallis test). Nuclear cataracts have a much higher positive or negative value than other cataract groups in the distribution of internal spherical aberrations by original value for each type of cataract. Other than this difference, the internal astigmatism and internal high order aberrations were not statistically significantly different.
CONCLUSIONS
The change in internal spherical aberrations of nuclear cataract from the original value was larger than cortical and posterior subcapsular cataract. Therefore, nuclear cataracts have much higher positive or negative values than other cataract groups.
MeSH Terms
Figure
-
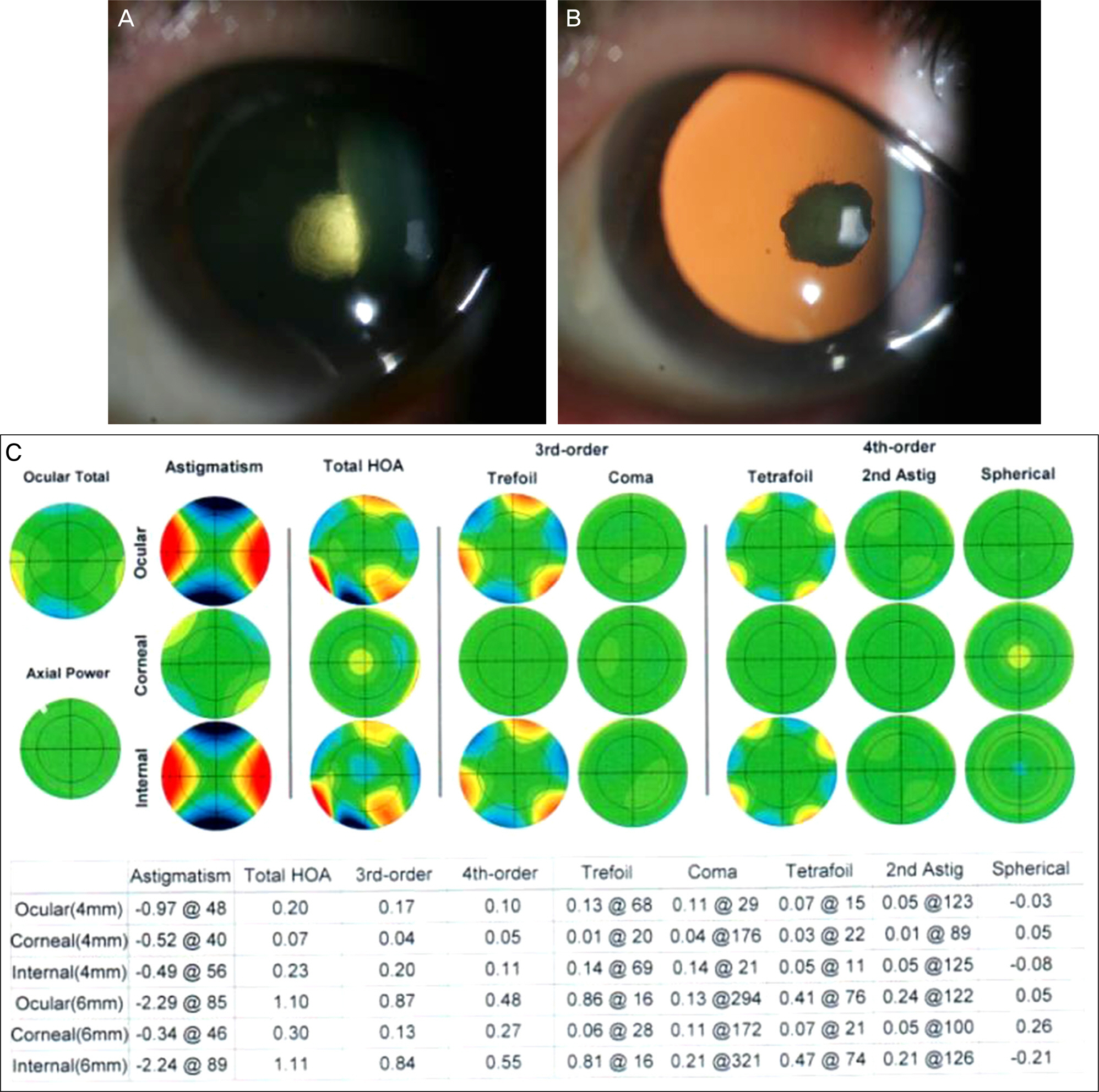
Figure 1. A case of posterior subcapsular cataract that was completely examined all of the aberration data using KR-1W. (A) A slit photo showed a posterior subcapsular cataract (NO1, NC2, C1, P4 in LOCS III score). (B) A photo with retroillumination. (C) The result of KR-1W wavefront aberrometer in this case. Astig = astigmatism; HOA = high order aberrations.
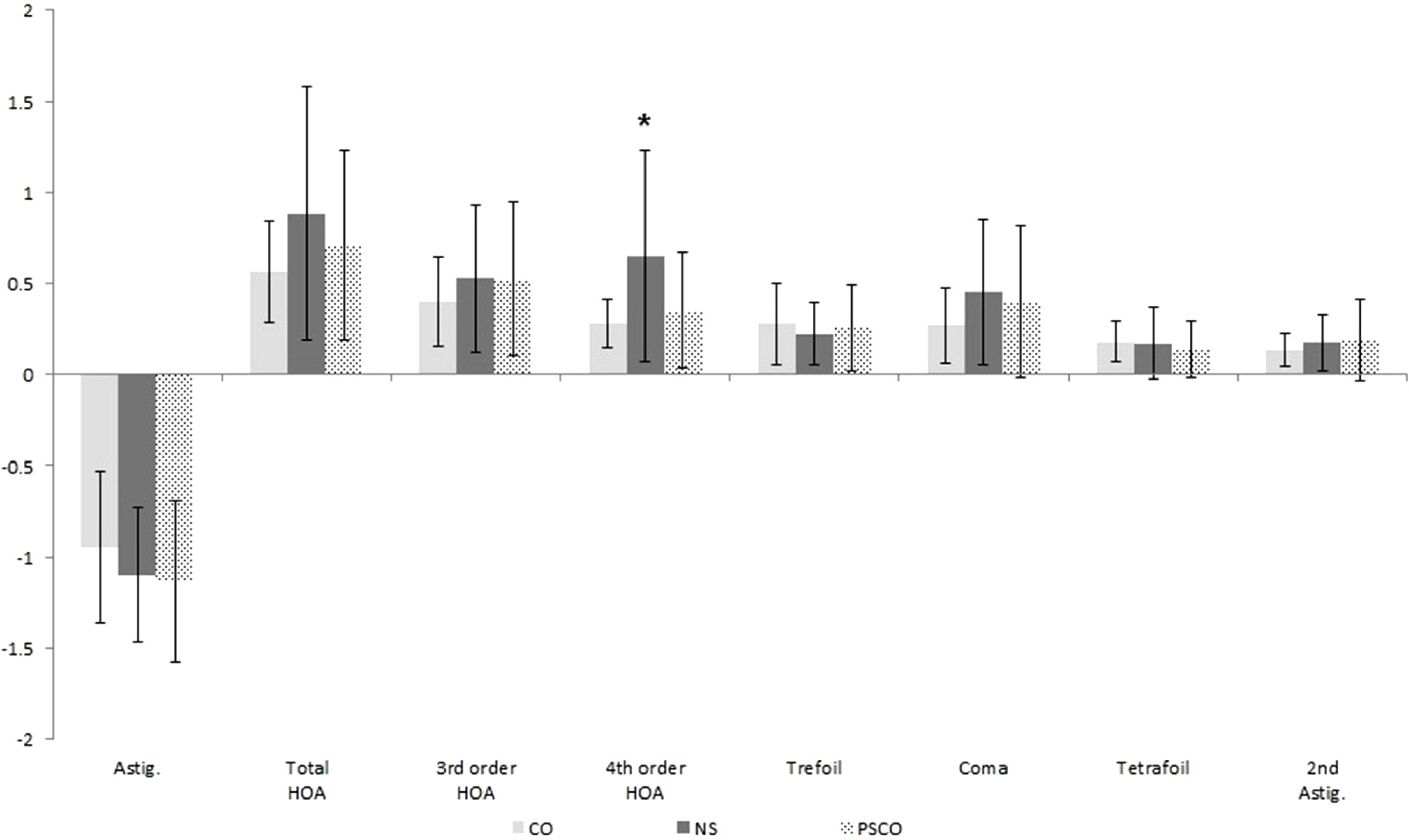
Figure 2. The average of internal astigmatism and internal high order aberrations on 6-mm diameter zone. The internal astigmatism and internal high order aberrations were not statistically significantly different except for 4th order high order aberrations ( p = 0.031, Kruskal-Wallis test). Astig = astigmatism; HOA = high order aberrations; CO = cortical opacity; NS = nuclear sclerosis; PSCO = posterior subcapsular opacity. *p < 0.05 based on Kruskal-Wallis test.

Figure 3. The average of internal spherical aberrations by original value and absolute value on 6-mm diameter zone. SA = spherical aberrations; Absolute = absolute value; Original = original value; CO = cortical opacity; NS = nuclear opacity; PSCO = posterior subcapsular opacity. * p < 0.017 based on Bonferroni-corrected post hoc Mann-Whitney U test. (A) The internal spherical aberrations by original value were not statistically significantly different. (B) The internal spherical aberrations by absolute value were statistically significantly different.
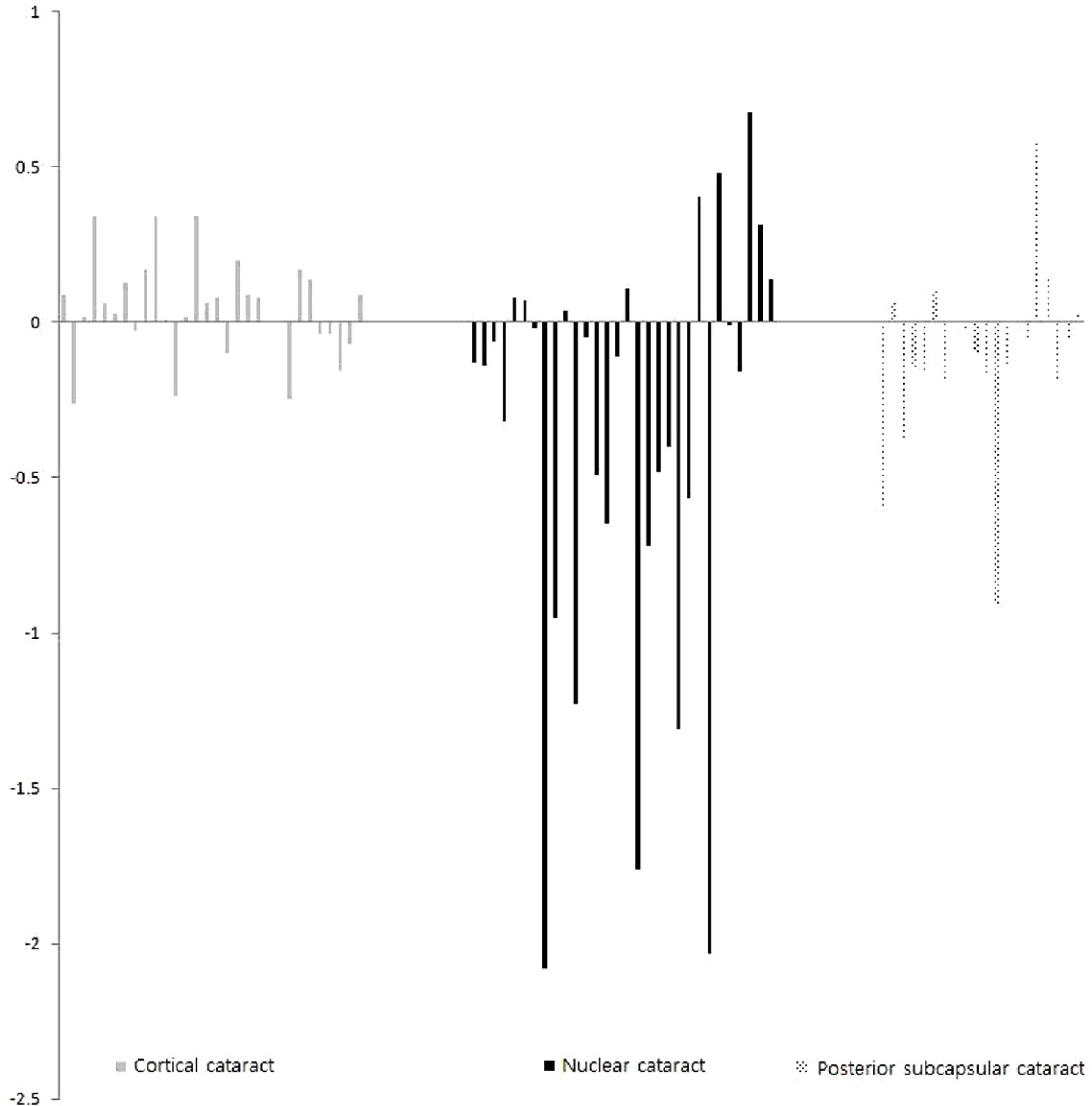
Figure 4. The distribution of internal spherical aberrations by original value for each type of cataract.

Figure 5. A case of nuclear cataract that had highly negative spherical aberration. The HOA map of ocular wavefront shows a delay of light (cool color) in the central pupillary area. In the color-coded map, cool color represents relatively delayed wavefront and a warm color represents relatively advanced wavefront. (A) A slit photo showed a nuclear cataract (NO4, NC4, C1 in LOCS III score). (B) The result of KR-1W wavefront aberrometer in this case. HOA = high order aberrations.
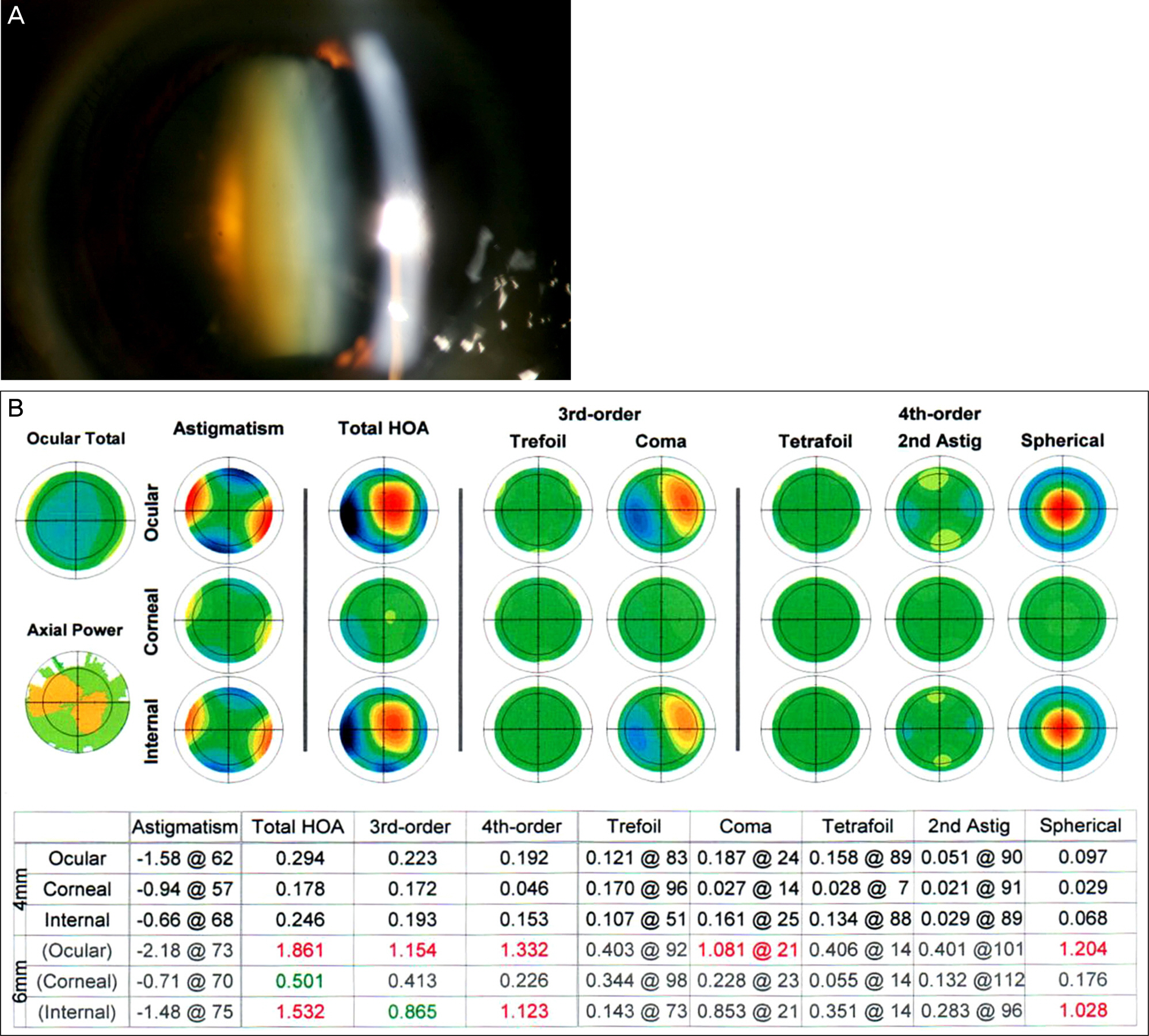
Figure 6. A case of nuclear cataract that had highly positive spherical aberration. The HOA map of ocular wavefront shows a delay of light (cool color) in the periphery. (A) A slit photo showed a nuclear cataract (NO5, NC5, C2 in LOCS III score). (B) The result of KR-1W wavefront aberrometer in this case. HOA = high order aberrations.
Reference
-
References
1. Porter J, Guirao A, Cox IG, Williams DR. Monochromatic aberrations of the human eye in a large population. J Opt Soc Am A Opt Image Sci Vis. 2001; 18:1793–803.
Article2. Applegate RA, Marsack JD, Ramos R, Sarver EJ. Interaction between aberrations to improve or reduce visual performance. J Cataract Refract Surg. 2003; 29:1487–95.
Article3. Kuroda T, Fujikado T, Ninomiya S, et al. Effect of aging on ocular light scatter and higher order aberrations. J Refract Surg. 2002; 18:S598–602.
Article4. Donnelly WJ 3rd, Pesudovs K, Marsack JD, et al. Quantifying scatter in Shack-Hartmann images to evaluate nuclear cataract. J Refract Surg. 2004; 20:S515–22.
Article5. Marcos S. Aberrations and visual performance following standard laser vision correction. J Refract Surg. 2001; 17:S596–601.
Article6. Tomidokoro A, Soya K, Miyata K, et al. Corneal irregular astigmatism and contrast sensitivity after photorefractive keratectomy. Ophthalmology. 2001; 108:2209–12.
Article7. Amano S, Amano Y, Yamagami S, et al. Age-related changes in corneal and ocular higher-order wavefront aberrations. Am J Ophthalmol. 2004; 137:988–92.
Article8. Rocha KM, Nosé W, Bottós K, et al. Higher-order aberrations of age-related cataract. J Cataract Refract Surg. 2007; 33:1442–6.
Article9. Chylack LT Jr, Wolfe JK, Singer DM, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993; 111:831–6.
Article10. Piñero DP, Juan JT, Alió JL. Intrasubject repeatability of internal aberrometry obtained with a new integrated aberrometer. J Refract Surg. 2011; 27:509–17.
Article11. Jeong JH, Kim MJ, Tchah HW. Clinical comparison of laser ray tracing aberrometer and shack-hartmann aberrometer. J Korean Ophthalmol Soc. 2006; 47:1911–9.12. Artal P, Guirao A, Berrio E, Williams DR. Compensation of corneal aberrations by the internal optics in the human eye. J Vis. 2001; 1:1–8.
Article13. Artal P, Guirao A. Contributions of the cornea and the lens to the aberrations of the human eye. Opt Lett. 1998; 23:1713–5.
Article14. Applegate RA, Sarver EJ, Khemsara V. Are all aberrations equal? J Refract Surg. 2002; 18:S556–62.
Article15. Kuroda T, Fujikado T, Maeda N, et al. Wavefront analysis in eyes with nuclear or cortical cataract. Am J Ophthalmol. 2002; 134:1–9.
Article16. Lee J, Kim MJ, Tchah H. Higher-order aberrations induced by nuclear cataract. J Cataract Refract Surg. 2008; 34:2104–9.
Article17. Alió JL, Schimchak P, Negri HP, Montés-Micó R. Crystalline lens optical dysfunction through aging. Ophthalmology. 2005; 112:2022–9.
Article18. Sachdev N, Ormonde SE, Sherwin T, McGhee CN. Higher-order aberrations of lenticular opacities. J Cataract Refract Surg. 2004; 30:1642–8.
Article19. Dubbelman M, Van der Heijde GL, Weeber HA. Change in shape of the aging human crystalline lens with accommodation. Vision Res. 2005; 45:117–32.
Article20. Dubbelman M, Van der Heijde GL, Weeber HA, Vrensen GF. Changes in the internal structure of the human crystalline lens with age and accommodation. Vision Res. 2003; 43:2363–75.
Article21. Yoo EJ, Kang SY, Kim HM, Song JS. The effects of pharmacologic pupil dilatation on ocular, corneal, and internal aberrations. J Korean Ophthalmol Soc. 2013; 54:581–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Optical Aberrations and Contrast Sensitivity between Monofocal and Multifocal Intraocular Lens
- Evaluation of Optical Quality Parameters and Ocular Aberrations in Multifocal Intraocular Lens Implanted Eyes
- Changes in High-order Aberrations after Phacotrabeculectomy Surgery
- Surgically Induced Astigmatism and Corneal Higher Order Aberrations in Microcoaxial and Conventional Cataract Surgery
- Higher-order Aberrations in Pseudophakia with Different Intraocular Lenses
