Medial and Lateral Canthal Tendon Laxity: An Evaluation of Patients with Involutional Entropion and Epiphora
- Affiliations
-
- 1Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea. shbaek6534@korea.ac.kr
- 2Department of Ophthalmology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 2215139
- DOI: http://doi.org/10.3341/jkos.2011.52.12.1385
Abstract
- PURPOSE
The degree of laxity of the medial and lateral canthal tendon in Korean subjects with and without involutional entropion and epiphora was evaluated in the present study.
METHODS
The present study included 180 normal subjects (360 eyes), 12 patients (15 eyes) with involutional entropion, and 41 patients (58 eyes) with epiphora. The degree of laxity of the medial and lateral canthal tendon, which grades the position of the inferior punctum, was measured using the lateral and medial distraction test.
RESULTS
The mean degree of medial and lateral canthal tendon laxity was 1.83/1.08 in normal subjects. A statistical difference was not observed between sexes, and the mean degree of laxity tended to be higher in older patients. The mean degree of laxity was 2.78/2.18 and 2.28/1.22 in the involutional entropion group and the epiphora group, respectively. The involutional entropion group and the epiphora group underwent endoscopic endonasal dacryocystitis (D), medial spindle procedure (M), and endoscopic endonasal dacryocystitis with the medial spindle procedure and/or the tarsal strip procedure (T). The mean degree of laxity was 1.84/1.04 in group D, 3.00/1.20 in group M, 2.33/2.00 in group D + T, 3.20/1.40 in group D + M and 3.50/2.00 in group D + T + M before surgery.
CONCLUSIONS
The results from the present study may aid in the selection of a basic treatment plan for Korean patients with involutional entropion or epiphora.
Figure
-

Figure 1. Lateral and medial distraction test for grading of medial and lateral canthal tendon laxity. (A) A photograph showing left lower lid laxity at resting state. (B) Lower lid lateral distraction test showing grade 2 medial canthal tendon laxity. (C) Lower lid medial distraction test showing grade 2 lateral canthal tendon laxity. The white arrow indicates the position of the punctum and the black arrow indicates the direction of the distraction test.
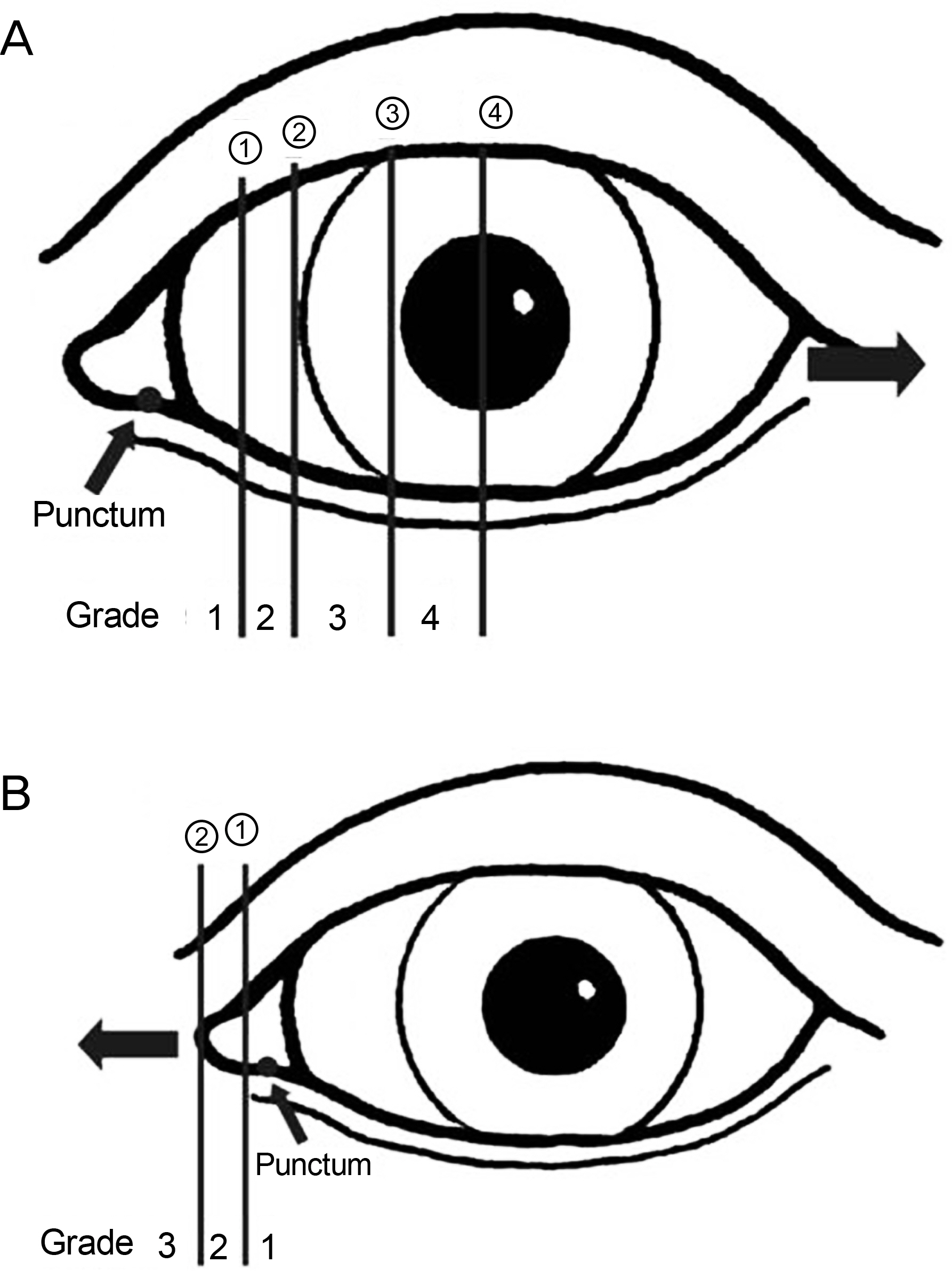
Figure 2. Medial and lateral canthal tendon laxity grades. (A) Grades of medial canthal tendon laxity. ①: Vertical midline between the medial limbus and the lateral border of the plica ②: Medial limbus ③: Vertical line of the medial border of the pupil ④: Vertical midline of the pupil. (B) Grades of lateral canthal tendon laxity. ①: Vertical midline of the caruncle ②: Medial canthal skin margin. The thin arrow indicates the position of the punctum and the thick arrow indicates the direction of the distraction test.

Figure 3. Mean canthal tendon laxity according to age range in the control group. ∗ p < 0.05 compared with the mean canthal tendon laxity in the 20-29 age group.
Cited by 1 articles
-
Effectiveness of Combined Surgery Simultaneously Correcting 3 Main Causes of Involutional Entropion
Sung Won Yang, Jin Hwan Park, Jun Sik Lee, Hwa Lee, Se Hyun Baek
J Korean Ophthalmol Soc. 2016;57(3):347-352. doi: 10.3341/jkos.2016.57.3.347.
Reference
-
References
1. Lew H, Lee SY, Kim SJ. The clinical evaluation on the patients complaining of epiphora. J Korean Ophthalmol Soc. 2000; 41:1112–7.2. Liu D, Stasior OG. Lower eyelid laxity and ocular symptoms. Am J Ophthalmol. 1983; 95:545–51.
Article3. Narayanan K, Barnes EA. Epiphora with eyelid laxity. Orbit. 2005; 24:201–3.
Article4. Stefanyszyn MA, Hidayat AA, Flanagan JC. The histopathology of involutional ectropion. Ophthalmology. 1985; 92:120–7.
Article5. Anderson RL, Hatt MU, Dixon R. Medial ectropion: a new technique. Arch Ophthalmol. 1979; 97:521–4.6. Ousterhout DK, Weil RB. The role of the lateral canthal tendon in lower eyelid laxity. Plast Reconstr Surg. 1982; 69:620–3.
Article7. Pottier F, El-Shazly NZ, El-Shazly AE. Aging of orbicularis oculi: Anatomophysiologic consideration in upper blepharoplasty. Arch Facial Plast Surg. 2008; 10:346–9.8. Snake RF. Relationship of senile ptosis to age. Ann Ophthalmol. 1984; 16:928–31.9. Goldberg B, Rabinovitch M. Connective tissue. Weiss L, Greep RO, editors. Histology. 4th ed.New York: McGraw-Hill;1977. p. 145–78.
Article10. Boboridis K, Bunce C, Rose GE. A comparative study of two procedures for repair of involutional lower lid entropion. Ophthalmology. 2000; 107:959–61.
Article11. Yoon JM, Kim SA, Roh JH. Clinical results of different surgical procedures in correcting involutional entropion. J Korean Ophthalmol Soc. 2008; 49:1877–87.
Article12. Fante RG, Elner VM. Transcaruncular approach to medial canthal tendon placation for lower eyelid laxity. Ophthal Plast and Reconstr Surg. 2001; 17:16–27.13. Barnes JA, Bunce C, Olver JM. Simple effective surgery for involutional entropion suitable for the general ophthalmologist. Ophthalmology. 2006; 113:92–6.
Article14. Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional entropion repair with fornix sutures and lateral tarsal strip procedure. Ophthal Plast Reconstr Surg. 2001; 17:281–7.
Article15. Detorakis ET, Zissimopoulos A, Katernellis G, et al. Lower eyelid laxity in functional acquired epiphora: Evaluation with quantitative scintigraphy. Ophthal Plast Reconstr Surg. 2006; 22:25–9.
Article16. Nowonski TS, Anderson RL. The medial spindle procedure for involutional medial ectropion. Arch Ophthalmol. 1985; 103:1750–3.17. Jordan DR, Anderson RL. The lateral tarsal strip revisited. The enhanced tarsal strip. Arch Ophthalmol. 1989; 107:604–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Correction of Involutional Entropion
- Effectiveness of Combined Surgery Simultaneously Correcting 3 Main Causes of Involutional Entropion
- Correction of Involutional Entropion by the Amount of Lower Eyelid Laxity
- Correction of Involutional Entropion by the Bowlegs Procedure
- Surgical Correction of Senile Entropion
