Multiple Serous Chorioretinopathy after Facial Herpes Zoster
- Affiliations
-
- 1Department of Ophthalmology, Chungbuk National University College of Medicine, Cheongju, Korea. cjbmed@naver.com
- KMID: 2213862
- DOI: http://doi.org/10.3341/jkos.2016.57.1.150
Abstract
- PURPOSE
To report a case of multiple serous chorioretinopathy after facial herpes zoster.
CASE SUMMARY
A 48-year-old male visited our clinic due to visual disturbance in the left eye which occurred 3 days after left facial pain and vesicles. Chemosis and multiple serous retinal detachments were found. The patient was diagnosed with multiple serous chorioretinopathy due to herpes zoster virus and was started on intravenous acyclovir at a dose of 10 mg/kg every 8 hours for 9 days and herpes eye ointment 5 times daily. After the initial treatment, oral prednisolone 60 mg was given daily for 6 days. Skin lesions were cleared, and abnormal fundus and visual acuity improved after treatment.
CONCLUSIONS
Ophthalmopathy including multiple serous chorioretinopathy should be considered in managing herpes zoster ophthalmicus patients.
MeSH Terms
Figure
-

Figure 1. Face photos showing facial herpes zoster. (A) Skin eruption corresponding to the dermatome of left ophthalmic branch of trigeminal nerve is observed. Nasal lesion shows Hutchinson's sign. (B) Oral mucosal erosion and pseudomembrane are observed at left upper soft plate.

Figure 2. Fundus photography, fluorescein angiography and optical coherence tomography showing multiple chorioretinopathy. (A) Multiple localized retinal detachments with subretinal fluid were found in macular and superior macular area. (B) Fluorescein an-giography shows multiple hyperfluorescent leaking points with localized serous detachment (arrowheads) between optic disc and macular area. (C) After treatment (two months later), fluorescein angiography shows no hyperfluorescence. (D) Multiple subretinal fluid and increased choroidal thickness were found. (E) After treatment, superior subretinal fluid moves downward to fovea. (F) After 1 month, subretinal fluid decreased. (G) After 2 months, subretinal fluid disappeared and there was no retinochoroidal inflammation.
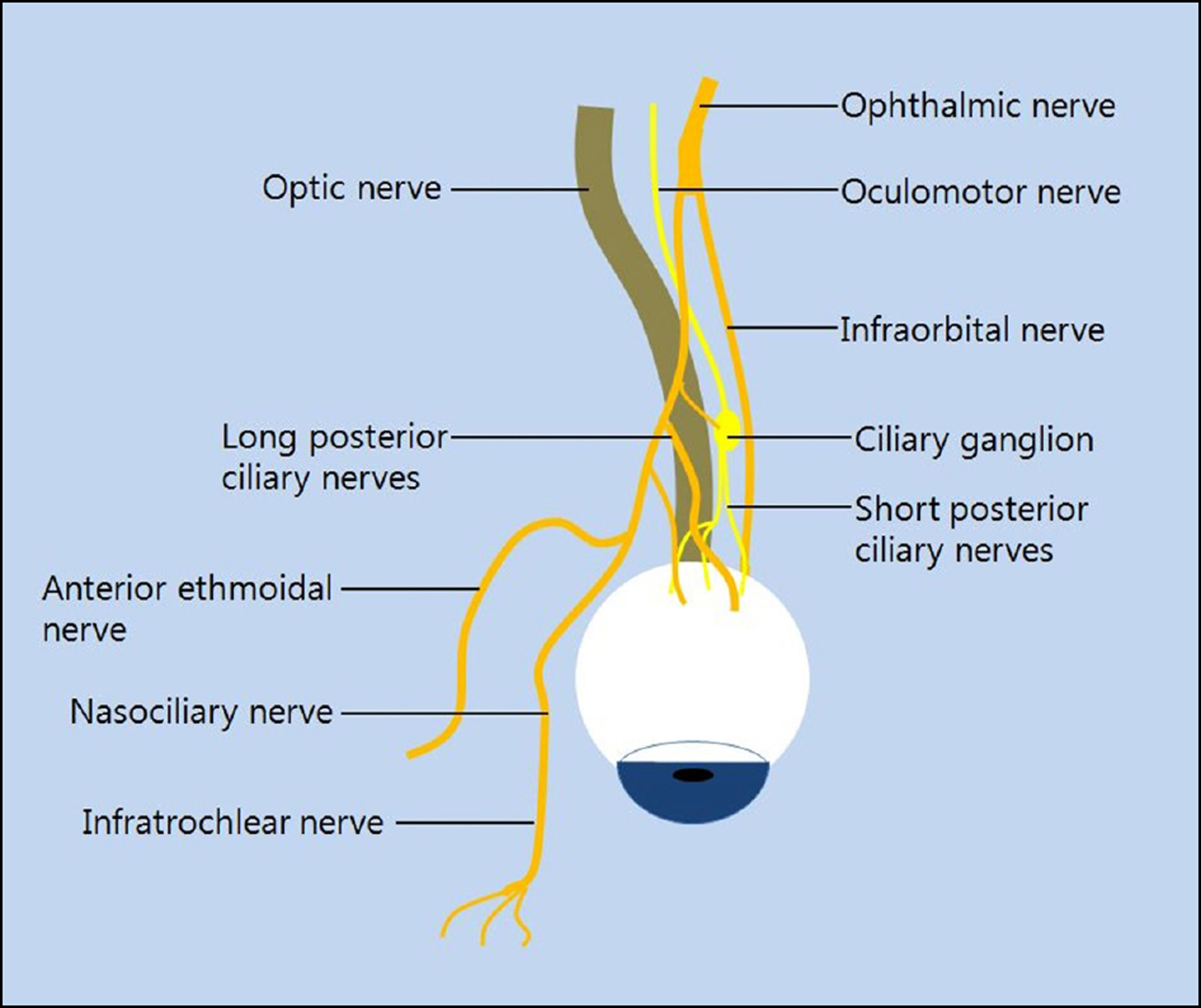
Figure 3. Anatomy of Ophthalmic branch in trigeminal nerve. Long posterior ciliary nerve and short posterior ciliary nerve cover posterior scleral area in the orbit.
Reference
-
References
1. Lee HK. Virus keratitis. Korea External Eye Disease Society. Cornea , editor. 3rd. Seoul: Ilchokak;2013. chap. 8.2. Liesegang TJ. Herpes zoster ophthalmicus natural history, risk fac-tors, clinical presentation, and morbidity. Ophthalmology. 2008; 115:(2 Suppl). S3–12.3. Lee HJ, Kim SY, Jung MS. The clinical characteristics of facial herpes zoster in Korean patients. J Korean Ophthalmol Soc. 2010; 51:8–13.
Article4. Chung YR, Chang YH, Kim DH. Yang HS. Ocular manifestations of herpes zoster ophthalmicus. J Korean Ophthalmol Soc. 2010; 51:164–68.
Article5. Lee WB, Liesegang TJ. Herpes zoster keratitis. Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 3rd. Philadelphia: Elsevier Mosby;2011. v. 1. chap. p. 40.
Article6. Park SH, Kim WJ, Yang SW. Kim MS. Herpes zoster ophthalmicus complicated by hyphema, glaucoma and external ophthalmoplegia. J Korean Ophthalmol Soc. 2007; 48:1573–8.
Article7. Kim M, Choi MY, Chae JB. Complicated ophthalmopathy in her-pes zoster ophthalmicus including vitreous opacity, retinal hemor-rhage and optic neuropathy. J Korean Ophthalmol Soc. 2013; 54:513–7.
Article8. Culbertson WW, Blumenkranz MS, Pepose JS. . Varicella zos-ter virus is a cause of the acute retinal necrosis syndrome. Ophthalmology. 1986; 93:559–69.
Article9. Zamora RL, del Priore LV. Storch GA. . Multiple recurrent branch retinal artery occlusions associated with varicella zoster virus. Retina. 1996; 16:399–404.
Article10. Gilden DH, Kleinschmidt-DeMasters BK, Wellish M. . Varicella zoster virus, a cause of waxing and waning vasculitis: the New England Journal of Medicine case 5-1995 revisited. Neurology. 1996; 47:1441–6.
Article11. Kim JY, Ahn M, Lee DW. Two cases of optic neuritis in herpes zos-ter ophthalmicus. J Korean Ophthalmol Soc. 2008; 49:1028–32.
Article12. Zaal MJ, Völker-Dieben HJ. DAmaro J. Prognostic value of Hutchinson’s sign in acute herpes zoster ophthalmicus. Graefes Arch Clin Exp Ophthalmol. 2003; 241:187–91.
Article13. Monica Evans. Anatomy of the Uvea. Yanoff M, Ducker JS, editors. Ophthalmology. 4th. Philadelphia: Elsevier Mosby;2014. chap. 7.1.
Article14. Dutton JJ. Atlas of Clinical and Surgical Orbital Anatomy, 2nd ed. London: Elsevier,. 2011; 51–82.15. Moorthy RS, Inomata H, Rao NA. Vogt-Koyanagi-Harada syndrome. Surv Ophthalmol. 1995; 39:265–92.
Article16. Greco A, Fusconi M, Gallo A. . Vogt-Koyanagi-Harada syndrome. Autoimmun Rev. 2013; 12:1033–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of Atypical Central Serous Chorioretinopathy with Bullous Retinal Detachment
- A Case of Herpes Zoster Oticus Involving Glossopharyngeal Nerve without Facial Nerve Palsy
- Herpes Zoster Oticus
- Herpes Zoster Oticus with Multiple Cranial Nerve Involvement: 2 Cases
- The prognostic factors of the facial nerve paralysis in herpes zoster oticus
