The Change of Severity of Epiblepharon after Induction of Total Intravenous Anesthesia without Muscle Relaxant
- Affiliations
-
- 1Department of Ophthalmology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. eyeyang@inje.ac.kr
- 2Therapeutics Center for Ocular Neovascular Disease, Inje University Busan Paik Hospital, Busan, Korea.
- 3Department of Anesthesiology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2212785
- DOI: http://doi.org/10.3341/jkos.2016.57.4.540
Abstract
- PURPOSE
To investigate the changes of epiblepharon by evaluating the severity of epiblepharon before and after induction of general anesthesia (GA) with a muscle relaxant and total intravenous anesthesia (TIVA) without a muscle relaxant.
METHODS
Thirteen pediatric patients (26 eyes) underwent surgery for epiblepharon under GA using a muscle relaxant and 19 pediatric patients (38 eyes) underwent surgery for epiblepharon under TIVA without a muscle relaxant. The severity of epiblepharon in each eye was scored according to skin-fold height (scored 1-4) and area of ciliocorneal touch (scored 1-3) while the patient was in the supine position before induction and after induction of GA.
RESULTS
Skin-fold height scores and ciliocorneal touch area scores decreased after induction of GA with a muscle relaxant (skin-fold height score before GA: 2.42 ± 0.86, after GA: 1.87 ± 0.88 p-value < 0.001; ciliocorneal touch area score before GA: 2.05 ± 0.70, after GA: 1.61 ± 0.68, p-value < 0.001). In the TIVA group, skin-fold height scores and ciliocorenal touch area scores were not statistically different before and after GA (skin-fold height score before GA: 2.23 ± 1.18, after GA: 2.38 ± 1.10, p-value = 0.212; ciliocorneal touch area score before GA: 2.06 ± 0.74, after GA: 1.94 ± 0.80, p-value = 0.161).
CONCLUSIONS
The change of epiblepharon severity was significantly reduced by induction of TIVA without a muscle relaxant and there was no recurrence of epiblepharon 3 months after surgery. When using TIVA without a muscle relaxant, the change of epiblepharon severity was reduced and thus, this method can help prevent its undercorrection.
Figure
-
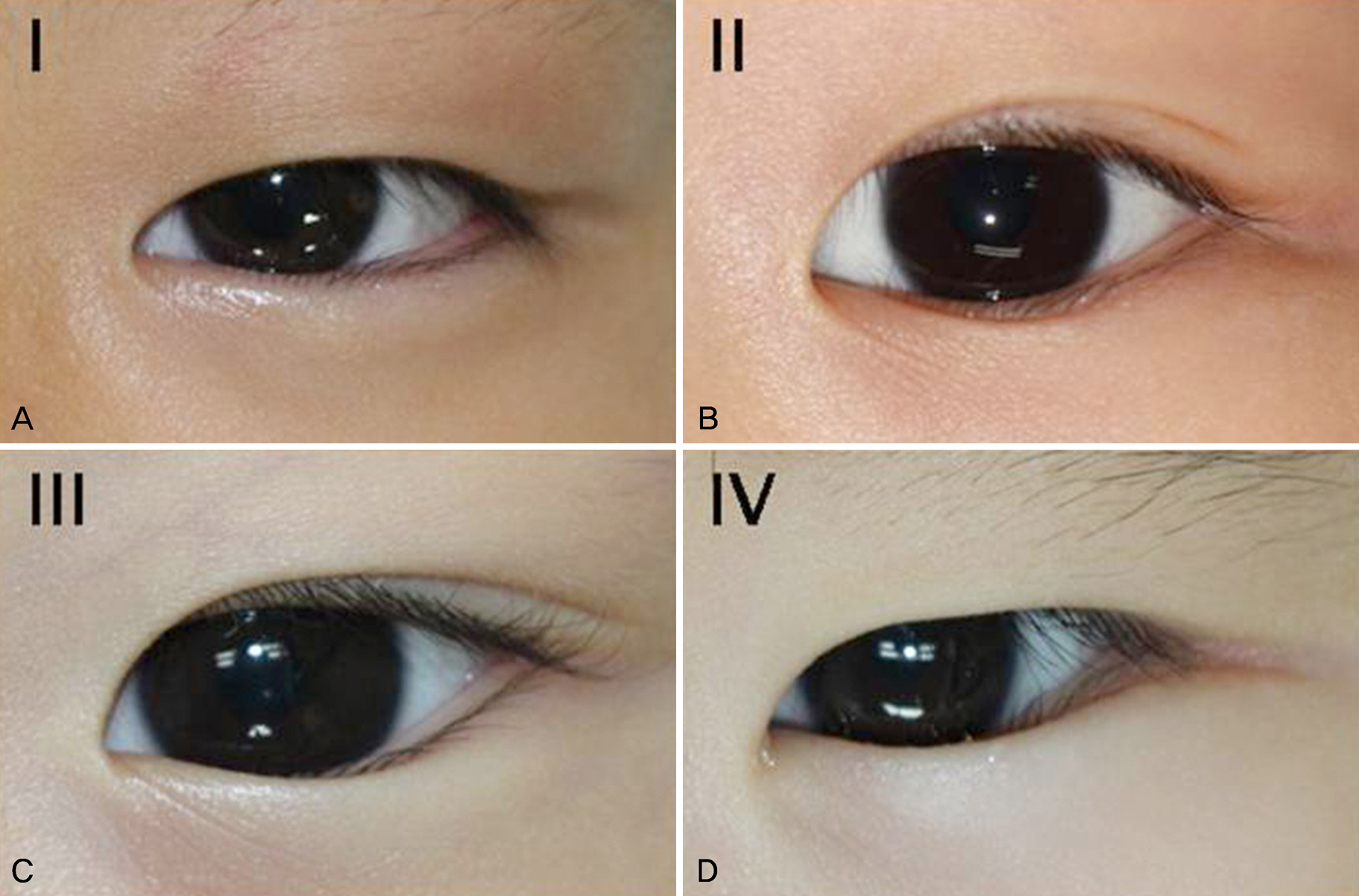
Figure 1. Classification of skin-fold height. According to the highest line of the skin fold located in the primary eye position opened as widely as possible. (A) Below the lower lid margin. (B) Just below or on the lower lid margin, without concealing the lid margin. (C) Above the lower lid margin with concealment of less than the medial one third of the lid margin. (D) Above the lower lid margin with concealment of more than the medial one third of the eyelid margin.

Figure 2. Classification of ciliocorneal touch. According to when the cilia touched the cornea. (A) Only in downgaze and not in primary gaze. (B) Less than the medial one half of the cornea. (C) More than one half of the cornea.
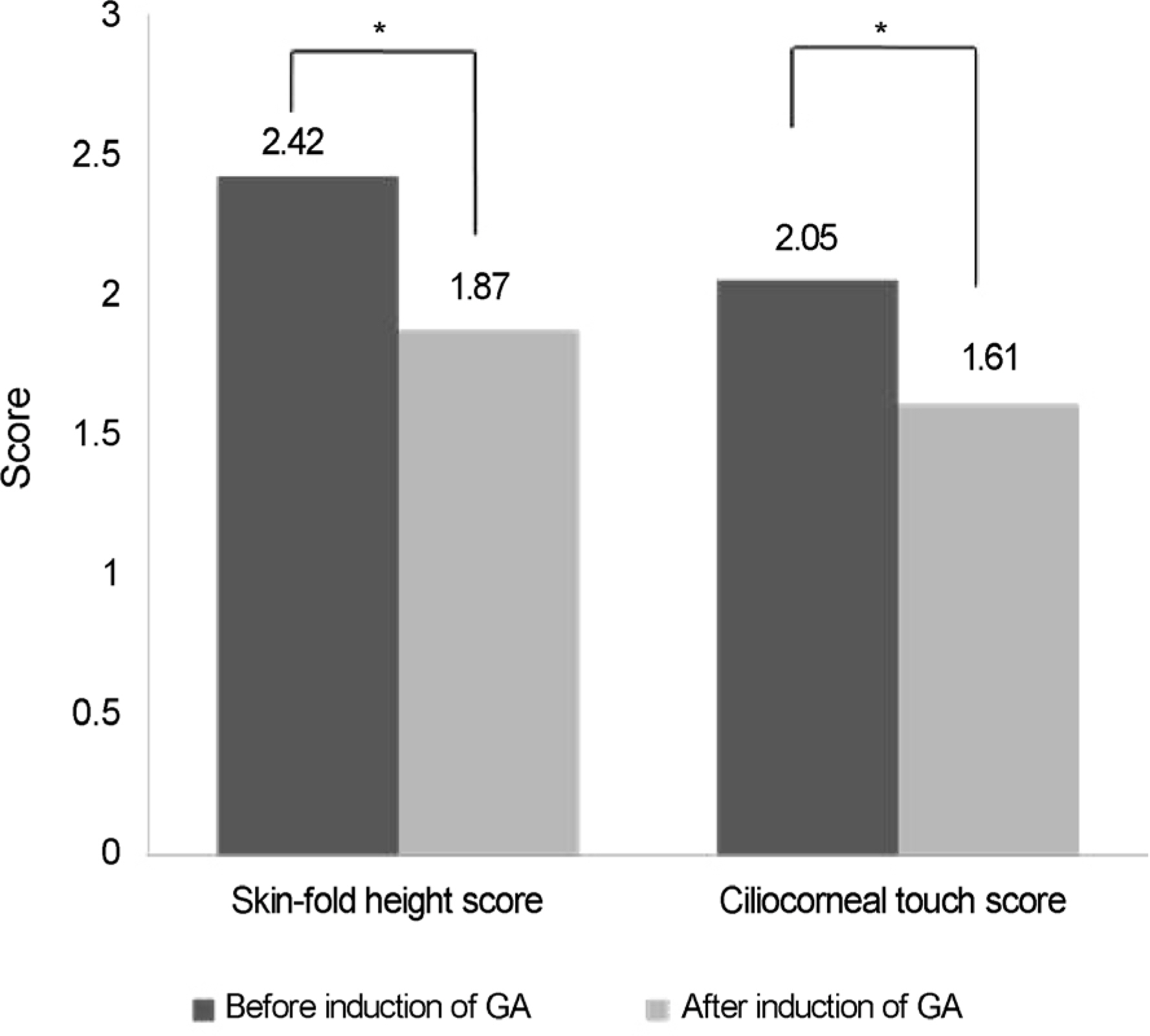
Figure 3. Comparison of degree of epiblepharon between the induction of GA in the muscle relaxant group. Before the induction of GA, the average value of the skin-fold height score was 2.42. After induction of GA, the average value of the skin-fold height score was 1.87. Before induction of GA, the average ciliocorneal touch score was 2.05. After induction of GA, the average ciliocorneal touch score was 1.61. Skin-fold height score and ciliocorneal touch score were significantly different before and after the induction of GA with muscle relaxant. GA = general anesthesia. *p<0.001.

Figure 4. Class proportion of skin-fold height score and ciliocorneal touch score between before and after the induction of GA with muscle relaxant. N = number of eyes; GA = general anesthesia.
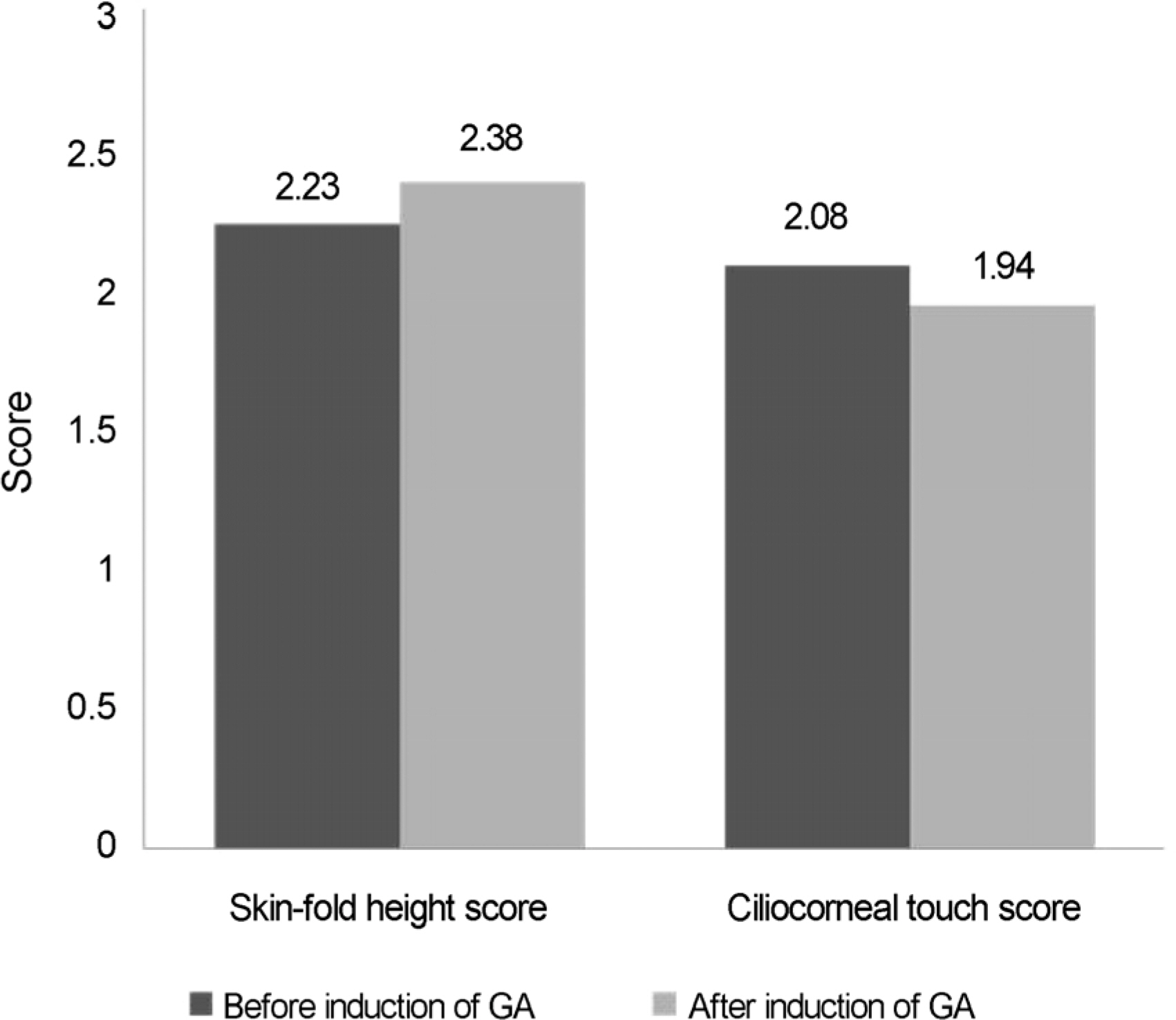
Figure 5. Comparison of degree of epiblepharon between induction of GA without muscle relaxant in the TIVA group. Before the induction of GA, the average skin-fold height score was 2.23. After the induction of GA, the average skin-fold height score was 2.38. Before the induction of GA, the average ciliocorneal touch score was 2.08. After the induction of GA, the average ciliocorneal touch score was 1.94. Skin-fold height score and ciliocorneal touch score were not significantly different before and after the induction of GA . TIVA = total intravenous anesthesia; GA = general anesthesia.
Reference
-
References
1. Noda S, Hayasaka S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol. 1989; 73:126–7.
Article2. Johnson CC. Epicanthus and epiblepharon. Arch Ophthalmol. 1978; 96:1030–3.
Article3. Levitt JM. Epiblepharon and congenital entropion. Am J Ophthalmol. 1957; 44:112–3.
Article4. Woo KI, Yi K, Kim YD. Surgical correction for lower lid epiblepharon in Asians. Br J Ophthalmol. 2000; 84:1407–10.
Article5. Jordan R. The lower-lid retractors in congenital entropion and epiblepharon. Ophthalmic Surg. 1993; 24:494–6.
Article6. Yang SW, Choi WC, Kim SY. Refractive changes of congenital entropion and epiblepharon on surgical correction. Korean J Ophthalmol. 2001; 15:32–7.
Article7. Quickert MH, Wilkes TD, Dryden RM. Nonincisional correction of epiblepharon and congenital entropion. Arch Ophthalmol. 1983; 101:778–81.
Article8. Kim KS. Neuromuscular block and reversal. J Korean Med Assoc. 2007; 50:1072–80.
Article9. Rhiu S, Yoon JS, Zhao SY, Lee SY. Variations in the degree of epiblepharon with changes in position and induction of general anesthesia. Graefes Arch Clin Exp Ophthalmol. 2013; 251:929–33.
Article10. Khwarg SI, Lee YJ. Epiblepharon of the lower eyelid: classification and association with astigmatism. Korean J Ophthalmol. 1997; 11:111–7.
Article11. Xue FS, Liao X, Tong SY, et al. Dose-response and time-course of the effect of rocuronium bromide during sevoflurane anaesthesia. Anaesthesia. 1998; 53:25–30.
Article12. Lowry DW, Mirakhur RK, McCarthy GJ, et al. Neuromuscular effects of rocuronium during sevoflurane, isoflurane, and intravenous anesthesia. Anesth Analg. 1998; 87:936–40.
Article13. Bock M, Klippel K, Nitsche B, et al. Rocuronium potency and recovery characteristics during steady-state desflurane, sevoflurane, isoflurane or propofol anaesthesia. Br J Anaesth. 2000; 84:43–7.
Article14. Wulf H, Ledowski T, Linstedt U, et al. Neuromuscular blocking effects of rocuronium during desflurane, isoflurane, and sevoflurane anaesthesia. Can J Anaesth. 1998; 45:526–32.
Article15. Harris EA, Lubarsky DA, Candiotti KA. Monitored anesthesia care (MAC) sedation: clinical utility of fospropofol. Ther Clin Risk Manag. 2009; 5:949–59.16. Kurdi MS, Theerth KA, Deva RS. Ketamine: current applications in anesthesia, pain, and critical care. Anesth Essays Res. 2014; 8:283–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes in Serum Electrolyte Concentration after Induction of Anesthesia with Intravenous Anesthetics and Nondepolarizing Muscle Relaxant
- Intravenous Anesthesia in Spinal Muscular Atrophy: A case report
- The Use of Total Intravenous Anesthesia Without Muscle Relaxation in Amyotrophic Lateral Sclerosis Patient
- The Influence of a Muscle Relaxant on Bispectral Index during the Propofol Induction of Anesthesia
- Application of Computers in Anesthesiolgy
