Right side fixation of sigmoid colon with a hepato-sigmoidocolic fistula in patient with hepatocellular carcinoma and midgut malrotation
- Affiliations
-
- 1Department of Surgery, Chosun University School of Medicine, Gwangju, Korea. kjkim@chosun.ac.kr
- 2Department of Pathology, Chosun University School of Medicine, Gwangju, Korea.
- 3Department of Gastroenterology, Chosun University School of Medicine, Gwangju, Korea.
- KMID: 2212472
- DOI: http://doi.org/10.4174/jkss.2013.84.4.256
Abstract
- The location of the sigmoid colon varies within the abdominal cavity, but its mesocolon is fixed to the left side. Right side fixation of the sigmoid colon is a very rare congenital positional anomaly. In addition, it has been reported that hepatocolic fistula is also a very rare disease that may present lower gastrointestinal bleeding. Here, the authors describe a case of a 71-year-old man who underwent surgery for hepato-sigmoidocolic fistula complicated by hepatocellular carcinoma and the right side fixation of the sigmoid colon.
Keyword
MeSH Terms
Figure
-
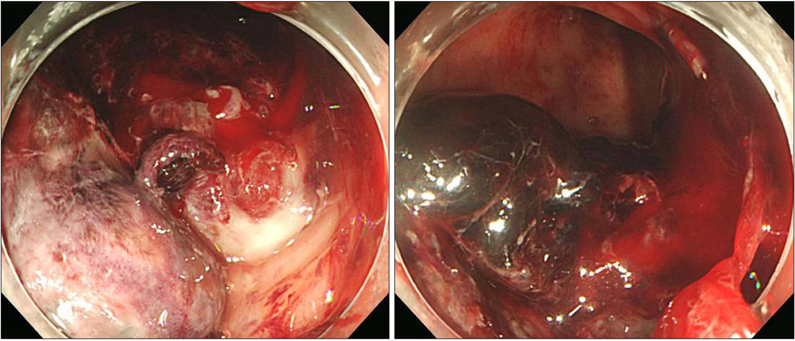
Fig. 1 Colonoscopic findings of the bleeding lesion of the colon. There was no active bleeding but 2 cm sized, solitary ulcerative lesion with dark-brown and dirty base at the sigmoid colon, about 30 cm from the anal verge, in which endoclips were applied (left side).

Fig. 2 Abdominopelvic computed tomographic scan showing a exophytic growth of the tumor from the right hepatic lobe. Endoclips applied in the bleeding lesion of the sigmoid colon during previous colonoscopy were visible very close to the hepatic tumor, but that finding was not noticed preoperatively.
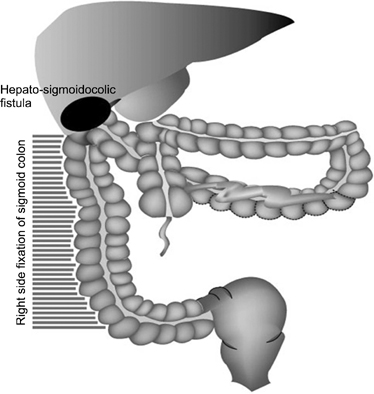
Fig. 3 Schematic drawing of the operation finding. Sigmoid colon and upper rectum were fixed to the right side of parietal peritoneum. Proximal part of the sigmoid colon was strongly adhered to the low surface of liver. And cecum and ascending colon was placed inner part of abdominal cavity and not fixed, consistent with midgut malrotation.
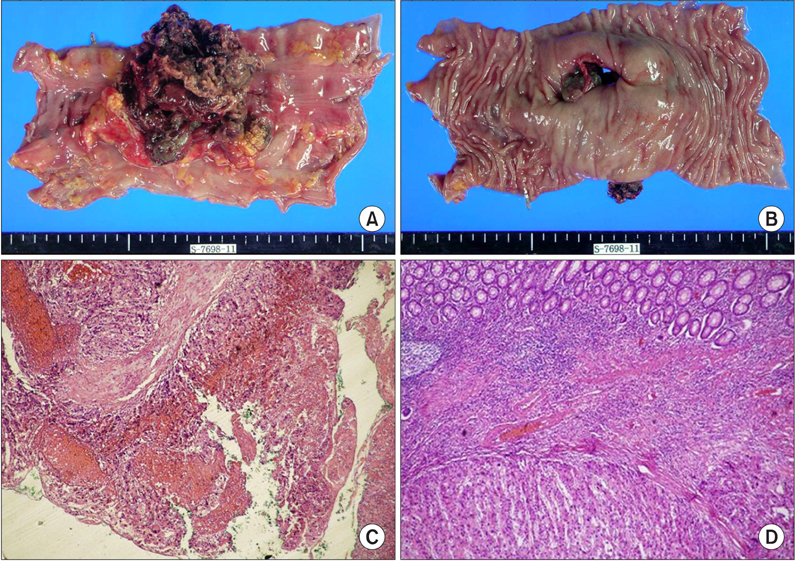
Fig. 4 Gross specimen and microscopic findings; (A) outer side of the gross specimen showing segmentally resected sigmoid colon together with hepatic tissue; (B) inner view of the gross specimen, showing the fistula opening; (C) microscopically in lower power field, tumor is seen in inked serosa margin (H&E, ×40); (D) in high power field, metastatic hepatocellular carcinoma is expanding from serosa to mucosa (H&E, ×100).
Reference
-
1. Malas MA, Aslankoc R, Ungor B, Sulak O, Candir O. The development of large intestine during the fetal period. Early Hum Dev. 2004. 78:1–13.2. Fiorella DJ, Donnelly LF. Frequency of right lower quadrant position of the sigmoid colon in infants and young children. Radiology. 2001. 219:91–94.3. Berkelhammer C, Janarthan B, Bhagavan M, Schreiber S. Hepatocolic fistula and lower GI bleeding in hepatoma. Am J Gastroenterol. 1996. 91:2625–2626.4. Ortiz H, Carmona JA, Perez-Cabanas I. Colohepatic fistula due to hydatid disease. Report of a case. Dis Colon Rectum. 1988. 31:546–547.5. Morris DL, Smith WD, Alexander-Williams J. Colohepatic fistula due to hydatid disease. World J Surg. 1983. 7:797–798.6. Bhattachayya B. Three cases of right-sided sigmoid colon. J Anat. 1926. 60(Pt 2):229–232.7. Wondrak E. Right-side fixation of the sigmoid colon. Rozhl Chir. 1957. 36:158–160.8. Schulz E, Bettenhaeuser K. On the roentgenologic differentiation of anomalies of the intestinal location (case of a fixed right location of an elongated sigmoid due to malrotation I). Fortschr Geb Rontgenstr Nuklearmed. 1963. 99:801–804.9. Komiyama M, Shimada Y. A case of a right-sided sigmoid colon. Kaibogaku Zasshi. 1991. 66:537–540.10. Singh Kalra TM, Mangla JC, Schwartz S, Lee JC. Hepatoma presenting as lower gastrointestinal bleeding. Am J Gastroenterol. 1977. 67:485–488.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Side Appendicitis with Abscess Caused by Midgut Malrotation Mimicked by Complicated Diverticulitis of Sigmoid Colon: A Case Report
- A Case of Combined Intrahepatic Portosystemic Shunt, Midgut Malrotation, and Renal Rotational Anomaly in an Adult Patient
- Appendico-Sigmoid Fistula Due to Appendicitis
- Colouterine Fistula Caused by Diverticulitis of the Sigmoid Colon
- Malrotation complicating Midgut Volvulus: Ultrasonographic Finding
