J Korean Ophthalmol Soc.
2009 Jun;50(6):864-869. 10.3341/jkos.2009.50.6.864.
The Effect of Posterior Subtenon Triamcinolone Injection in Panretinal Photocoagulation Induced Visual Dysfunction of Diabetic Retinopathy
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, College of Medicine, The Catholic University of Korea, Seoul, Korea. parkyh@catholic.ac.kr
- KMID: 2212363
- DOI: http://doi.org/10.3341/jkos.2009.50.6.864
Abstract
-
PURPOSE: To evaluate the efficacy of a prophylactic posterior sub-Tenon's capsule injection of Triamcinolone acetonide (TA) against macular edema and visual dysfunction by panretinal photocoagulation (PRP) in patients with severe nonproliferative and proliferative diabetic retinopathy.
METHODS
Thirty-eight eyes of 19 patients who have diabetic retinopathy without macular edema and whose retinopathy was bilateral and symmetrical were evaluated. Triamcinolone was injected into the posterior sub-Tenon's capsule in one eye of the patients and nothing was injected in the other eye as a control. Two weeks later, PRP was performed every other week for 4 sessions on both eyes in all patients. The clinical course of visual acuity and macular edema was monitored for up to approximately 6 months after the initial PRP.
RESULTS
There was no statistically significant difference of visual acuity before PRP in the 2 groups (p>0.05), and there was no macular edema in any patient. For a follow-up period of 6 months, visual dysfunction was more severe in the TA-injected eye than the control. However, the difference was not statistically significant (p>0.05) throughout the follow-up period except at the 20-week time point. On the other hand, macular edema occurred in 2 eyes (10.5%) of the TA-injected group, and in 4 eyes (21.1%) of the control group. IOP elevation as a complication caused by TA-injection occurred in 2 eyes (10.5%). However, IOP was controlled successfully by anti-glaucomatic eye drops.
CONCLUSIONS
Posterior sub-Tenon's capsule injection of Triamcinolone is a safe and effective treatment modality for preventing PRP-induced visual dysfunction and macular edema.
Keyword
MeSH Terms
Figure
-
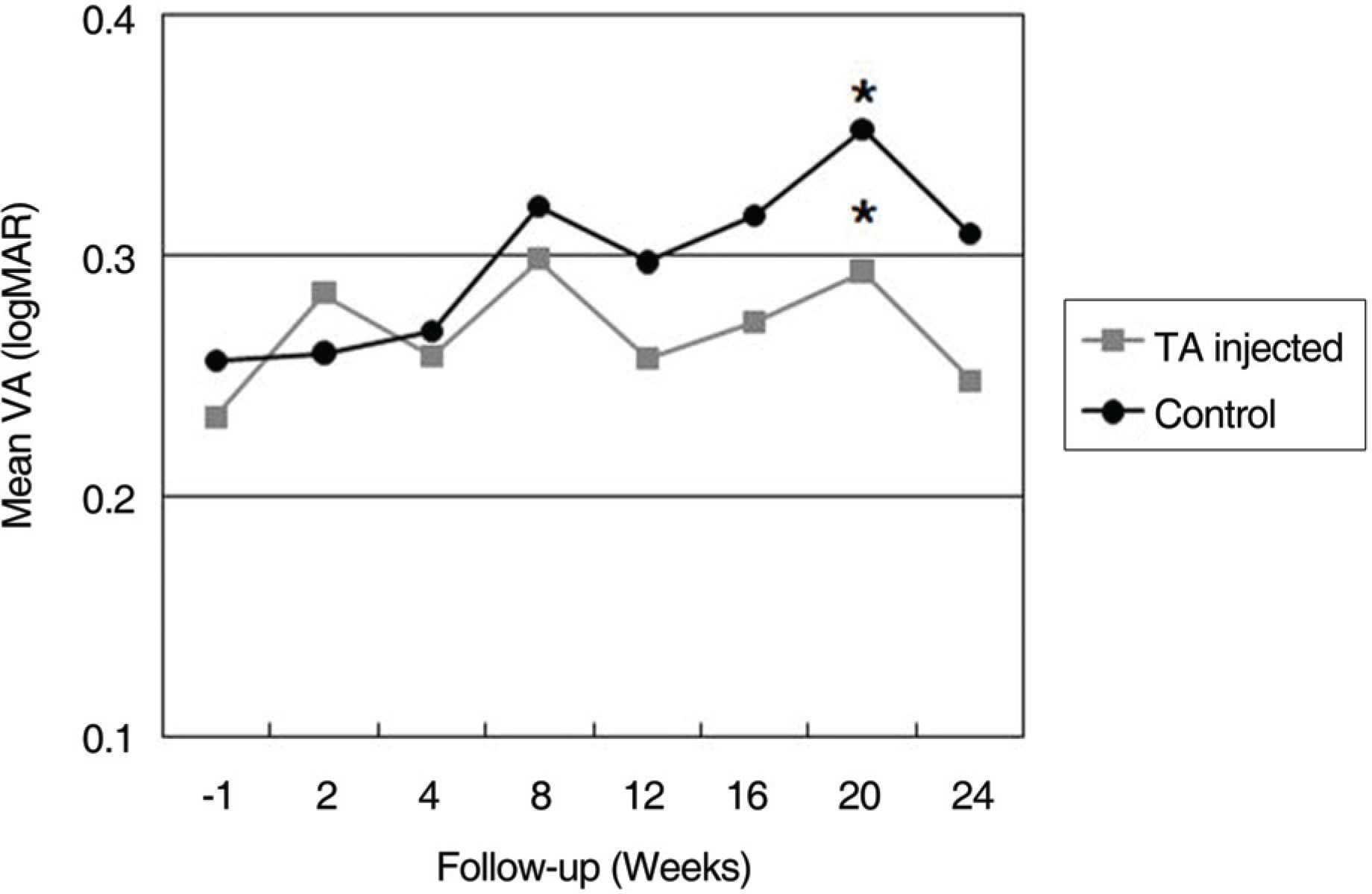
Figure 1. Line graph illustrating of the clinical course of logarithm of the minimum angle of resolution (logMAR) visual acuity between the TA-inejcted and control eyes. There was not statistically significant difference between two groups before TA injection and after 2 weeks. TA-injected group shows relatively good vision than control group through the follow-up period. But the difference was not statistically significant (p>0.05) except at 20 weeks follow-up time point (p<0.05). (* statistically significant difference between the TA-injected and control eyes at the point)
Reference
-
References
1. Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy, ETDRS report number 9. Ophthalmology. 1991; 98:766–85.2. Early Treatment Diabetic Retinopathy Study Research Group. Early treatment diabetic retinopathy study design and baseline patient characteristics, ETDRS report number 7. Ophthalmology. 1991; 98:741–56.3. Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol. 1976; 81:383–96.4. The Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical applications of DRS findings. DRS Report No 8. Ophthalmology. 1981; 88:583–600.5. Verma LK, Vivek MB, Kumar A, et al. A prospective controlled trial to evaluate the adjunctive role of posterior subtenon triamcinolone in the treatment of diffuse diabetic macular edema. J Ocular Pharmacol Ther. 2004; 20:277–84.
Article6. Meyer-Schwickerath GR, Schott K. Diabetic retinopathy and photocoagulation. Am J Ophthalmol. 1968; 66:597–603.
Article7. Martidis A, Duker JS, Greenberg PB, et al. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology. 2002; 109:920–7.
Article8. Tano Y, Chandler D, Machemer R. Treatment of intraocular proliferation with intravitreal injection of triamcinolone acetonide. Am J Ophthalmol. 1980; 90:810–6.
Article9. Ozdek S, Bahceci UA, Gurelik G, Hasanreisoglu B. Posterior subtenon and intravitreal triamcinolone acetonide for diabetic macular edema. J Diabetes Complications. 2006; 20:246–51.10. Bakri SJ, Kaiser PK. Posterior subtenon triamcinolone for refractory diabetic macular edema. Am J Ophthalmol. 2005; 139:290–4.11. Bonini-Filbo MA, Jorge R, Barbosa JC, et al. Intravitreal injection versus subtenon's infusion of triamcinolone acetonide for refractory diabetic macular edema: a randomized clinical trial. Ophthalmol Vis Sci. 2005; 46:3845–9.12. Cardillo JA, Melo LA, Cost RA, et al. Comparison of intravitreal versus posterior subtenon's capsule injection of triamcinolone acetonide for diffuse diabetic macular edema. Ophthalmology. 2005; 112:1557–63.
Article13. Lee YH, Kim CG. Intravitreal triamcinolone acetonide injection for treatment of macular edema. J Korean Ophthalmol Soc. 2004; 45:2055–63.14. Zacks DN, Johnson MW. Combined intravitreal injection of triamcinolone acetonide and panretinal photocoagulation for concomitant diabetic macular edema and proliferative diabetic retinopathy. Retina. 2005; 25:135–40.
Article15. Henricsson M, Heijl A. The effect of panretinal laser photocoagulation on visual acuity, visual fields and on subjective visual impairment in preproliferative and early proliferative diabetic retinopathy. Acta Ophthalmol. 1994; 72:570–5.
Article16. Gentile RC, Stegman Z, Liebmann JM, et al. Risk factors for choroidal effusion after panretinal photocoagulation. Ophthalmology. 1996; 103:827–32.17. Lam DS, Chan CK, Tang EW, et al. Intravitreal triamcinolone for diabetic macular edema in Chinese patients: six-month prospective longitudinal pilot study. Clin Experiment Ophthalmol. 2004; 32:569–72.18. Islam MS, Vemon SA, Negi A. Intravitreal triamcinolone will cause posterior subcapsular cataract in most eyes with diabetic maculopathy within 2 years. Eye. 2006; 17:1–3.
Article19. Moshfeghi DM, Kaiser PK, Scott IU, et al. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003; 136:791–6.
Article20. Nelson ML, Tennant MT, Sivalingam A, et al. Infectious and presumed noninfectious endophthalmitis after intravitreal triamcinolone acetonide injection. Retina. 2003; 23:686–91.
Article21. Roth DB, Chieh J, Spirn MJ, et al. Noninfectious endophthalmitis associated with intravitreal triamcinolone injection. Arch Ophthalmol. 2003; 121:1279–82.
Article22. Jonas JB, Kreissig I, Degenring RF. Endophthalmitis after intravitreal injection of triamcinolone injections. Arch Ophthalmol. 2003; 121:1279–82.23. Craig JH, Gray NH. The effects of posterior subtenon injection of triamcinolone acetonide in patients with intermediate uveitis. Am J Ophthalmol. 1995; 120:55–64.24. Kang SB, Park YH. The Combined Effect of Subtenon Triamcinolone Injection and Panretinal Photocoagulation on Diabetic Retinopathy. J Korean Ophthalmol Soc. 2008; 49:71–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Combined Effect of Subtenon Triamcinolone Injection and Panretinal Photocoagulation on Diabetic Retinopathy
- Intravitreal versus Posterior Subtenon Injection of Triamcinolone Acetonide for Diabetic Macular Edema
- Short-term Effect of Intravitreal Bevacizumab Injection Preventing Panretinal Photocoagulation-Induced Macular Edema in Proliferative Diabetic Retinopathy
- Intravitreal and Additional Posterior Subtenon Triamcinolone Injection in Diabetic Macular Edema
- Macular Thickness and Visual Acuity Before and After Panretinal Photocoagulation in Severe Diabetic Retinopathy
