Urachal cyst presenting with huge abscess formation in adults
- Affiliations
-
- 1Department of Surgery, Migrant Worker's Hospital, Seoul, Korea.
- 2Department of Pathology, Seoul Medical Center, Seoul, Korea.
- 3Department of Surgery, Seoul Medical Center, Seoul, Korea. shindonggue@naver.com
- KMID: 2212321
- DOI: http://doi.org/10.4174/jkss.2012.83.4.254
Abstract
- Urachal disease, a disorder where embryonic remnant of the cloaca and the allantois present after birth as a midline fibrous cord, is usually detected in infancy and childhood. But urachal disease in adults is rare. We report a case of a huge abscess derived from a urachal cyst in an adult. A 52-year-old man presented with peri-umbilical distension and abdominal pain for 2 weeks. Ultrasonography and abdominal computed tomography scan demonstrated a huge abscess derived from the abdominal wall. After prompt incision and drainage, the remaining abscess cavity was removed completely under general anesthesia. Pathologic report was consistent with urachal duct cyst, and the patient was discharged in a week without complication.
Keyword
MeSH Terms
Figure
-

Fig. 1 Computed tomography showed huge abscess containing fluid and gas below umbilicus.

Fig. 2 The operative findings. Abscess cavity and urachus was completely removed. Thin fibrous band was observed between abscess cavity and the middle of mesentery, but there was no communication with small bowel.
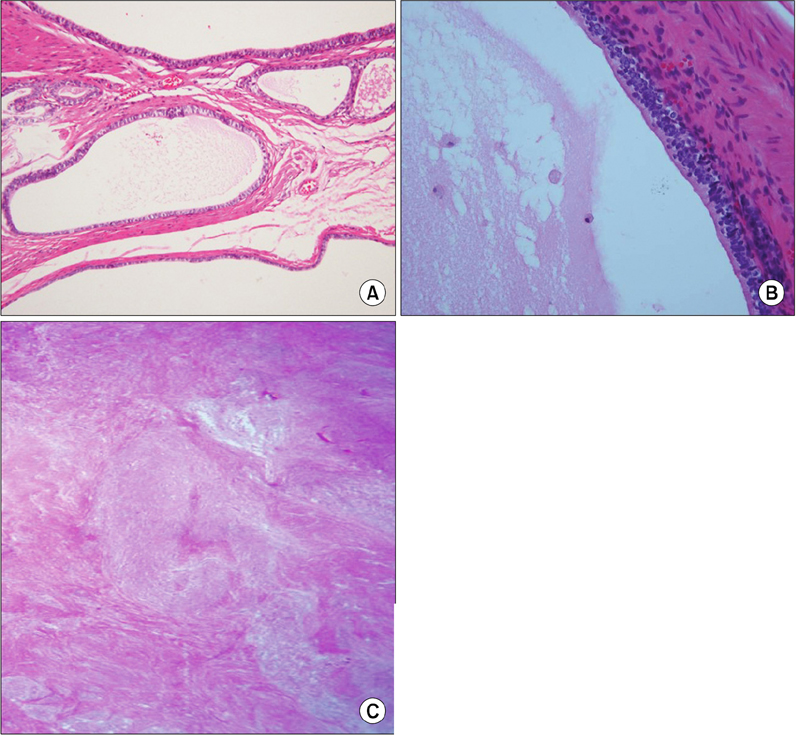
Fig. 3 Microscopic findings. (A) Variable sized multilocular cysts or ducts lined by urothelial, cuboidal or columnar epithelium. Some large cysts were lined by flattened epithelium (H&E, ×20). (B) The cystic lumen contains some histiocytes and lymphocyte infiltration is observed in the lining epithelium (H&E, ×40). (C) Low power view shows multiple inflammatory cell infiltration and surrounding fibrosis around fistula tract of umbilicus (H&E, ×4).
Reference
-
1. Moore KL. Moore KL, editor. The urogenital system. The developing human: clinically oriented embryology. 1982. 3rd ed. Philadelphia: Saunders;255–297.2. Mesrobian HG, Zacharias A, Balcom AH, Cohen RD. Ten years of experience with isolated urachal anomalies in children. J Urol. 1997. 158(3 Pt 2):1316–1318.3. Spataro RF, Davis RS, McLachlan MS, Linke CA, Barbaric ZL. Urachal abnormalities in the adult. Radiology. 1983. 149:659–663.4. Yiee JH, Garcia N, Baker LA, Barber R, Snodgrass WT, Wilcox DT. A diagnostic algorithm for urachal anomalies. J Pediatr Urol. 2007. 3:500–504.5. Goldman IL, Caldamone AA, Gauderer M, Hampel N, Wesselhoeft CW, Elder JS. Infected urachal cysts: a review of 10 cases. J Urol. 1988. 140:375–378.6. Berman SM, Tolia BM, Laor E, Reid RE, Schweizerhof SP, Freed SZ. Urachal remnants in adults. Urology. 1988. 31:17–21.7. Walsh SA, Weiss RM. Case report: persistent dysuria and a suprapubic mass in a 3-year-old boy. Curr Opin Pediatr. 2002. 14:647–648.8. Pesce C, Costa L, Musi L, Campobasso P, Zimbardo L. Relevance of infection in children with urachal cysts. Eur Urol. 2000. 38:457–460.9. Mesrobian HG, Zacharias A, Balcom AH, Cohen RD. Ten years of experience with isolated urachal anomalies in children. J Urol. 1997. 158(3 Pt 2):1316–1318.10. Lee SI, Kim SS, Moon HY. Laparoscopic extraperitoneal resection of urachal cyst. J Korean Surg Soc. 2010. 78:267–269.
