Macular Pseudohypopyon in Bilateral Terson's Syndrome
- Affiliations
-
- 1Department of Ophthalmology, Soonchunhyang University College of Medicine, Seoul, Korea. wismile@unitel.co.kr
- KMID: 2211913
- DOI: http://doi.org/10.3341/jkos.2009.50.1.167
Abstract
- PURPOSE
To report a case of a macular pseudohypopyon in the right eye in bilateral Terson's syndrome.
CASE SUMMARY
During a right eye vitrectomy of a 56-year-old female patient who showed bilateral Terson's syndrome with subarachnoid hemorrhage, a macular pseudohypopyon was observed. In an oval-shaped subinternal limiting membrane cyst (4x2 diameter size disc) including the central fovea, white exudates with fluid levels were present. The macular pseudohypopyon in the right eye was suspected to have occurred during the absorption of the subinternal limiting membrane hemorrhage. In the left eye, white exudates were clustered in the central fovea. In the right eye, the central fovea was above the fluid level of the pseudohypopyon, and corrected visual acuity was 1.0 after 6 months. Two months after the operation, the pseudohypopyon was absorbed.
MeSH Terms
Figure
-
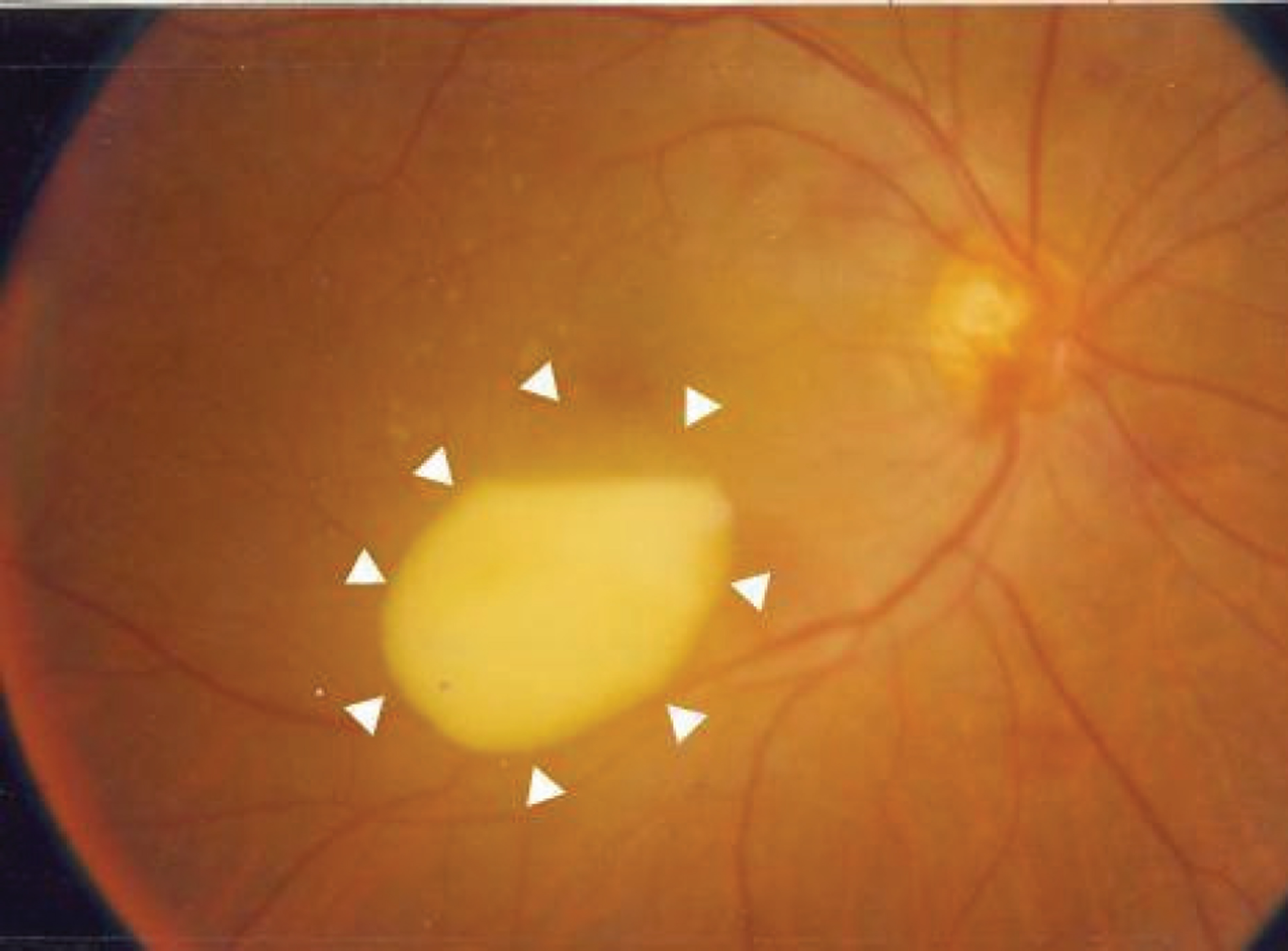
Figure 1. Fundus photograph of the right eye during operation. It shows a splint hemorrhage on the disc and a dense subinternal limiting membrane exudate with fluid level (pseudohypopyon).

Figure 2. Postoperative fundus photographs of the right eye (A) and left eye (B) after 3 weeks, and the right eye (C) and left eye (D) after 2 months. (A) The pseudohypopyon diminished at the posterior pole. (B) The wedge-shaped hemorrhage was absorbed at the posterior pole. The white exudates were presented at margin and base of previous hemorrhage. (C) The pseudohypopyon vanished at the posterior pole. (D) The dense subinternal limiting membrane exudates disappeared. However, the retinal atrophic lesion and pigmentation was found on the previous hemorrhage area.

Figure 3. Postoperative fundus photographs of the right eye (A) and left eye (B), and optical coherence tomography by line scanning on the macula of the right eye (C) and left eye (D) after 6 months. (A) Subretinal exudates on the macula were seen. (B) The foveal atrophic change was significant and retinal pigment epithelial thickening was noted on the macula. (C) The normal macula was observed. (D) The photoreceptor layer was lost, and retinal pigment epithelial thickening was noted on the macula.
Reference
-
References
1. Sharma MC, Lai WW, Shapiro MJ. Pseudohypopyon following intravitreal triamcinolone acetonide injection. Cornea. 2004; 23:398–9.
Article2. Chan JH, Dua HS, Tranos PG. . Pseudohypopyon due to malignant infiltration of the anterior chamber in multiple myeloma. Eye. 2005; 19:112–3.
Article3. Kraushar MF, Margolis S, Morse PH, Nugent ME. Pseudo-hypopyon in Best’s vitelliform macular dystrophy. Am J Ophthalmol. 1982; 94:30–7.
Article4. Ouano DP, Brucker AJ, Saran BR. Macular pseudohypopyon from secondary syphilis. Am J Ophthalmol. 1995; 119:372–4.
Article5. Naseripour M. Shields CL, Shields JA, Guyer DR. Pseudo-hypopyon of orange pigment overlying a stable choroidal nevus. Am J Ophthalmol. 2001; 132:416–7.6. Fish RH, Territo C, Anand R. Pseudohypopyon in unilateral acute idiopathic maculopathy. Retina. 1993; 13:26–8.
Article7. Gross JG. Endogenous Aspergillus-induced endophthalmitis. Successful treatment without systemic antifungal medication. Retina. 1992; 12:341–5.8. Cogan DG. Neurology of the visual system. Springfield: Charles C Thomas;1966. p. 184–93.
Article9. Tsuhihiko O, Takashi K, Yoshinori D. . A case report suggesting the mechanism of vitreous hemorrhage. Ophthal-mology. 2001; 108:1654–6.10. Toosi SH, Malton M. Terson's syndrome significance of ocular findings. Ann Ophthalmol. 1987; 19:7–12.11. Ogawa T, Kitaoka T, Dake Y, Amemiya T. Terson syndrome: a case report suggesting the mechanism of vitreous hemorr-hage. Ophthalmology. 2001; 108:1654–6.12. Friedman SM, Margo CE. Bilateral subinternal limiting membrane hemorrhage with Terson syndrome. Am J Ophthalmol. 1997; 124:850–1.
Article13. Meier P, Schmitz F, Wiedemann P. Vitrectomy for pre-macular hemorrhagic cyst in children and young adults. Graefes Arch Clin Exp Ophthalmol. 2005; 243:824–8.
Article14. De Maeyer K, Van Ginderdeuren R, Postelmans L. . Sub inner limiting membrane hemorrhage: Causes and treatment with vitrectomy. Br J Ophthalmol. 2007; 91:869–72.15. Glatt H, Machemer R. Experiemental subretinal hemorrhage in rabbits. Am J Ophthalmol. 1982; 94:762–3.16. Toth CA, Morse LS, Hjelmeland LM, Landers MB III. Fibrin directs early retinal damage after experimental subretinal hemorrhage. Arch Ophthalmol. 1991; 109:723–9.
Article17. Ritland JS, Syndalen P, Eide N. . Outcome of vitrectomy in patients with Terson syndrome. Acta Ophthalmol Scand. 2002; 80:172–5.
Article18. Kim US, Yu SY, Kwak HW. Incidence and postoperative visual outcome of Terson's syndrome. J Korean Ophthalmol Soc. 2002; 43:2451–6.19. Fahmy J. Vitreous hemorrhage in subarachnoid hemorrhage. Terson's syndrome. Acta Ophthalmol. 1972; 50:137–43.20. Kim HC, Kwon SI, Kim HK. The effect of intravitreal injection of tPA and C3 F8 gas in submacular hemorrhage. J Korean Ophthalmol Soc. 2000; 41:400–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full Thickness Macular Holes Associated with Terson Syndrome
- Incidence and Postoperative Visual Outcome of Terson's Syndrome
- Pseudohypopyon in Vitelliform Macular Dystrophy
- Terson's Syndrome due to Subarachnoid Hemorrhage after Rupture of MCA Bifurcation Aneurysm
- Incidence, Treatment and Prognosis of Terson's Syndrome
