J Korean Soc Spine Surg.
2003 Mar;10(1):64-68. 10.4184/jkss.2003.10.1.64.
Disturbance of Toe Walking in Mid-lumbar Spinal Stenosis: Three Cases Report
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Institute for Medical Science, Chonbuk National University Hospital, Chonju, Korea. kysong@moak.chonbuk.ac.kr
- 2Department of Orthopedic Surgery, Soonchun Hospital, Soonchun, Korea.
- KMID: 2209706
- DOI: http://doi.org/10.4184/jkss.2003.10.1.64
Abstract
- We report three cases of toe walking disturbance due to mid-lumbar spinal canal stenosis, which is a condition rarely reported in the literature. A severe bilateral S1 root lesion, associated with spinal stenosis at L3-4, is described. The diagnosis was obtained using computed tomography myelography (CTM) and magnetic resonance imaging (MRI). The findings at L5-S1 were minimal, and did not justify the patients clinical symptoms (disturbance of toe walking), but a detailed radiological evaluation revealed severe spinal stenosis at L3-4, which was assumed to be the cause of the S1 nerve root compression. A decompressive laminectomy, posterolateral fusion and posterior stabilization were performed. The pain and claudication had disappeared at the last follow-up evaluation, but the clinical symptom associated with the S1 root (toe walking) had not recovered.
MeSH Terms
Figure
-

Fig. 1. Anteroposterior and lateral radiography demonstrating myelographic block at L3-4 and L4-5 level.
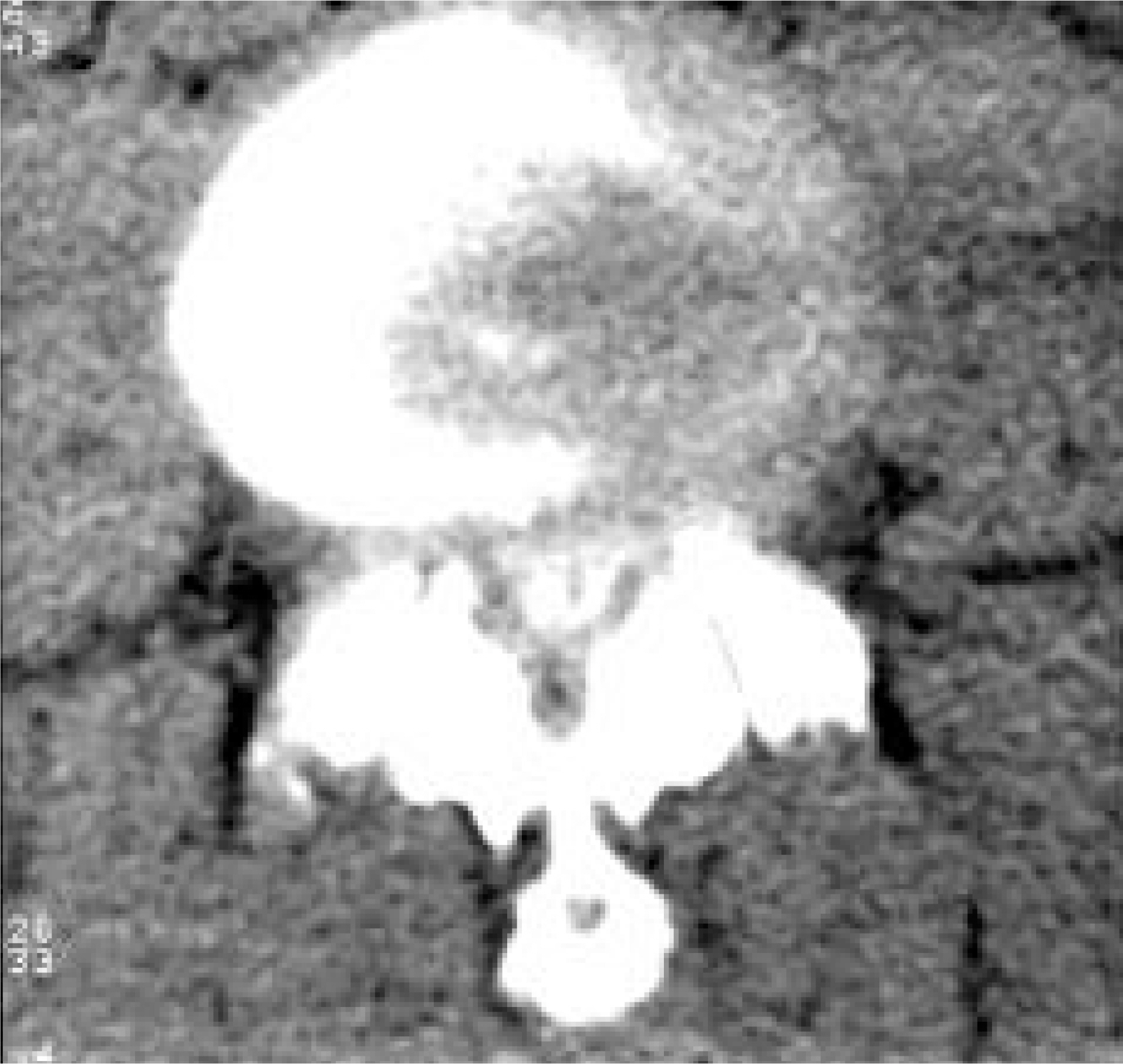
Fig. 2. An axial image of the L3-4 myelo-CT shows central and foraminal stenosis with hypertrophied facet joint, ligamentum flava and its disc extrusion.
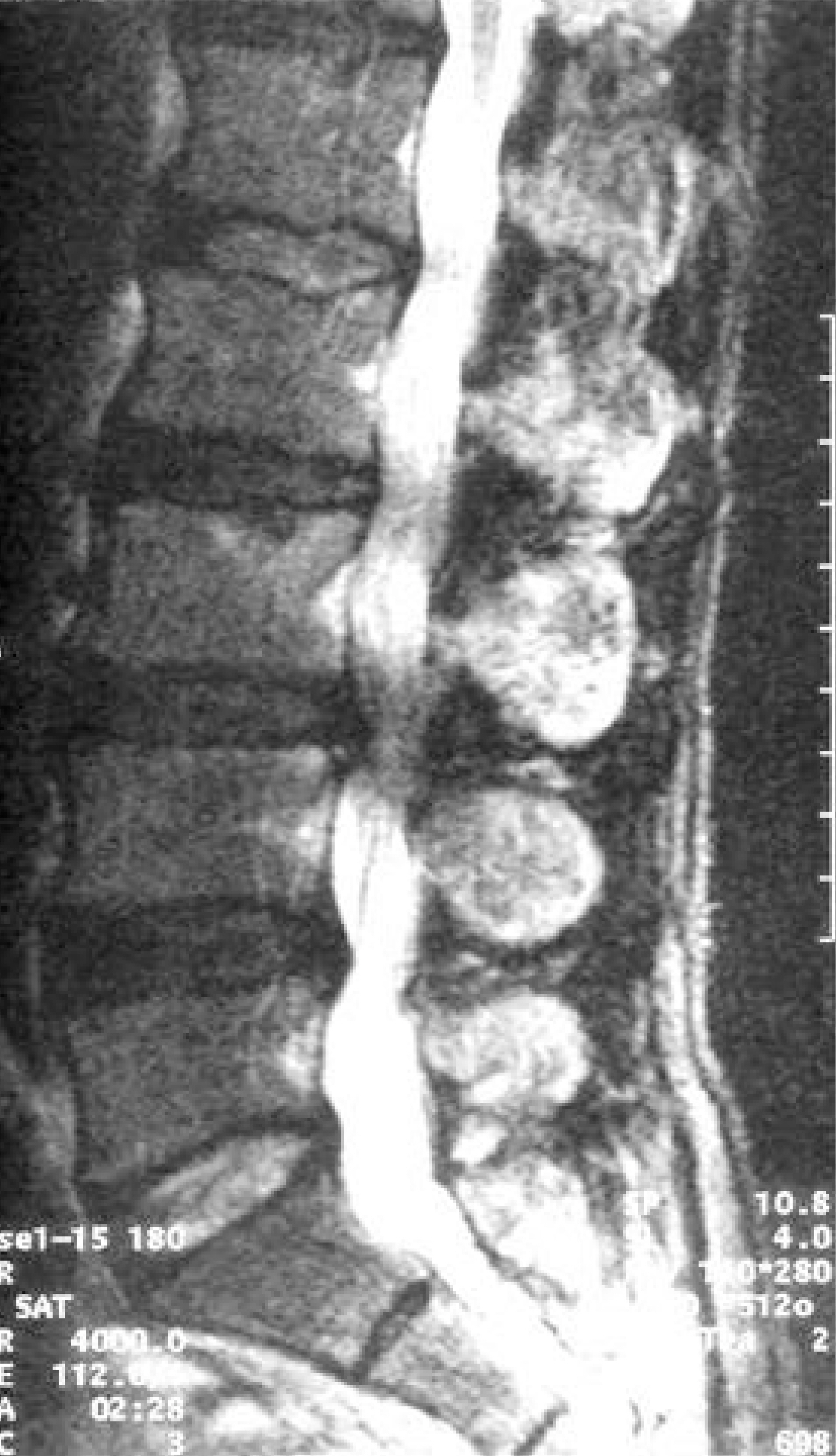
Fig. 3. A T2-weighted sagittal image showing degenerated discs with canal stenosis at L3-4 and L4-5.
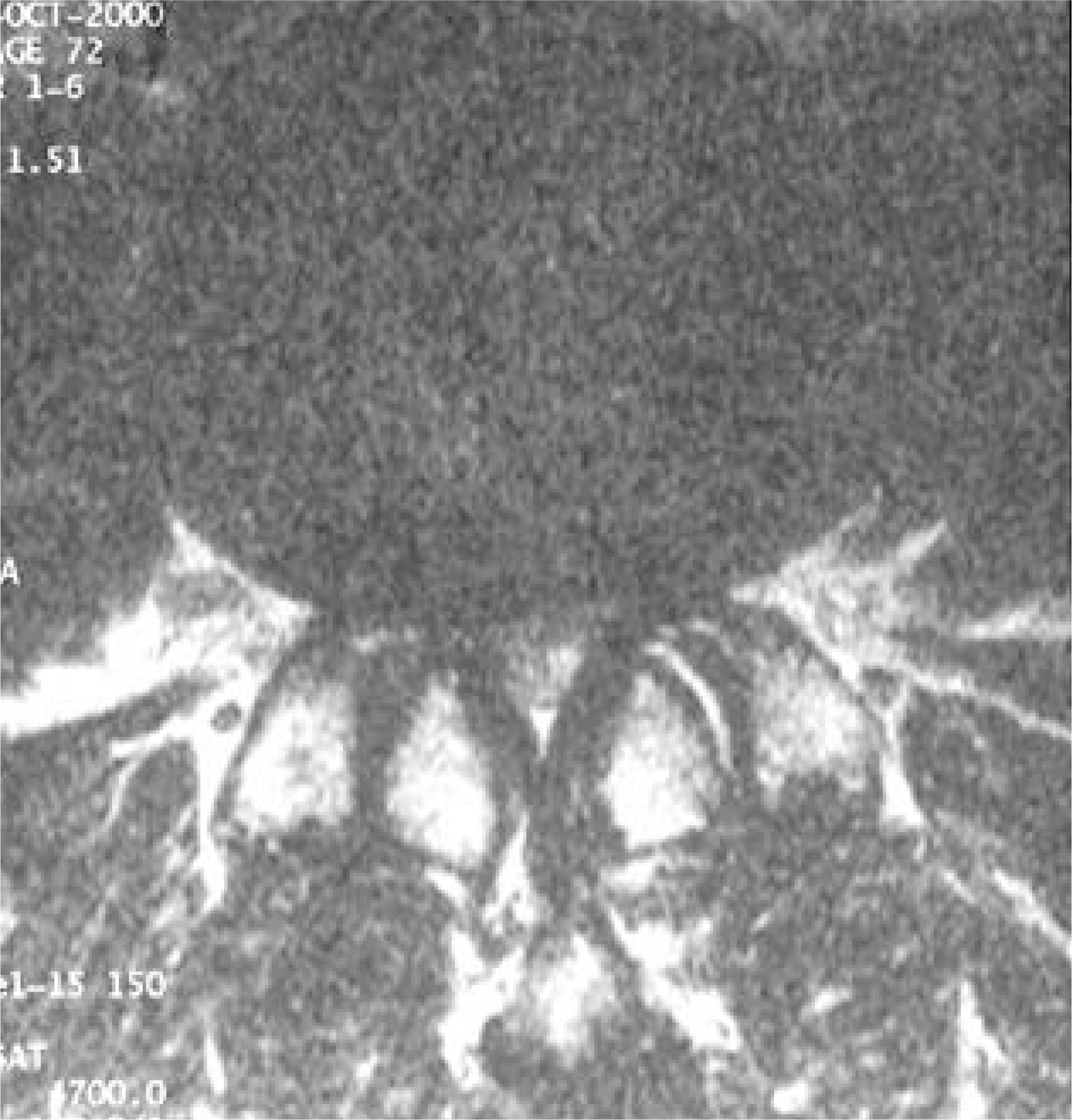
Fig. 4. An axial image of the MRI show stenosis of central portion of spinal canal by hypertrophied facet joint, ligamentum flava and extruded disc at L3-4 level.

Fig. 5. Solid union with stable posterior stabilization were achieved using plain radiography, and neurogenic claudication improved but toe gait disturbance was persist-ed on 24 months follow-up evaluation.
Reference
-
1). Grabias S. The treatment of spinal stenosis: Current con -cepts review. J Bone Joint Surg,. 62-A:308–13. 1980.2). Hashimoto T., Kaneda K., Abumi K. Relati ons hip between traumatic spinal canal stenosis and neurological deficits in thoracolumbar burst fractures. Spine,. 13:1268–72. 1988.3). Martinelli TA., Wisel SW. Epidemiology of spina stenosis. Instructional Course of Lecture. XLI:179–181. 1992.4). Ooy Y., Mita F., Satoh Y. Myeloscopic study on lum -bar spinal canal stenosis with special reference to inter -mittent claudication. Spine,. 15:544–9. 1990.5). Porter RW. Spinal stenosis and neurologic claudication. Spine,. 21:2046–52. 1996.6). Porter RW., Ward D. Cauda equina dysfunction: The significance of two level pathology. Spine,. 17:9–15. 1992.7). Shirado O., Matsukawa S., Kaneda K. Herniation of the disc between the first and second lumbar vertebrae with a monoradiculopathy of the fifth lumbar nerve root. J Bone Joint Surg,. 72-A:1422–6. 1996.8). Wall EJ., Cohen MS., Abitbol JJ., Garfin SR. Orga -nization of intrathecal nerve roots at the level of the conus medullaris. J Bone Joint Surg,. 78-A:1495–99. 1990.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Coexisting Cervical and Lumbar Spinal Stenosis
- Dynamic Effects on F wave Parameters and SEPs in Lumbar Canal Stenosis
- Result of Pedicle Screw Fixation in Lumbar Stenosis with: A Comparison of Degenerative Type Lumbar Stenosis with Spondylolisthetic type Lumbar Stenosis
- Y-Angle Stenosis of Lumbar Spine: New Concept of Lumbar Stenosis
- Atypical Guillain-Barre Syndrome Misdiagnosed as Lumbar Spinal Stenosis
